2 Development and Eruption of the Teeth
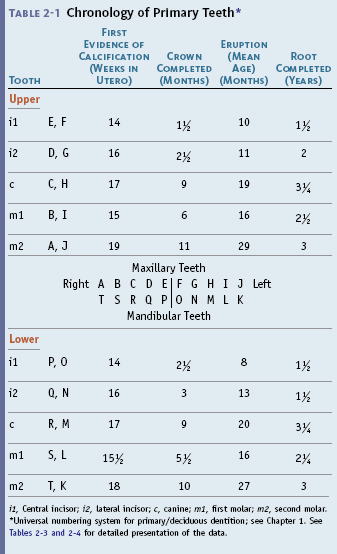

i1, Central incisor; i2, lateral incisor; c, canine; m1, first molar; m2, second molar.
* Universal numbering system for primary/deciduous dentition; see Chapter 1. See Tables 2-3 and 2-4 for detailed presentation of the data.
Table 2-2 Chronology of Permanent Teeth*
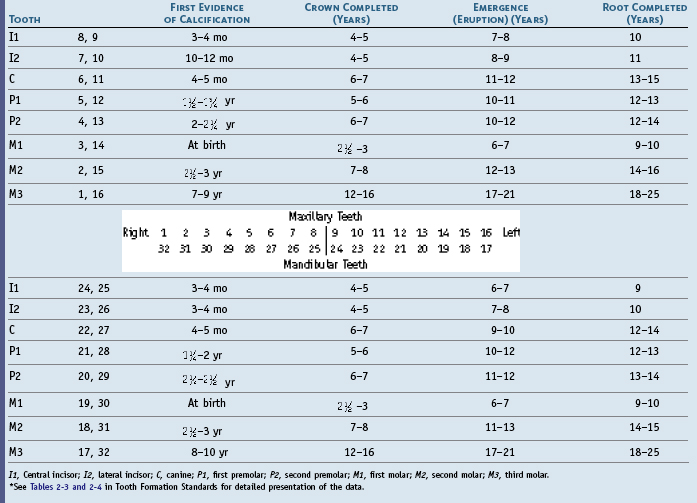
I1, Central incisor; I2, lateral incisor; C, canine; P1, first premolar; P2, second premolar; M1, first molar; M2, second molar; M3, third molar.
* See Tables 2-3 and 2-4 in Tooth Formation Standards for detailed presentation of the data.
Clinical Considerations
It must be kept in mind that the dental practitioner sees in a “normal” healthy mouth not only the clinical crowns of the teeth surrounded by the gingival tissues, but also the number, shape, size, position, coloration, and angulations of the teeth; the outlines of the roots of the teeth; occlusal contacts; evidence of function and parafunction; and phonetics and esthetics. Most of the parts of the teeth that are hidden by the gingiva can be visualized radiographically. This can also be done by using a periodontal probe to locate the depth of normal or pathologically deepened gingival crevices or a dental explorer to sense the surfaces of the teeth within the gingival crevice apical to the free gingival margin as far as the epithelial attachment of the gingiva to the enamel. In addition, in pathologically deepened crevices, tooth surfaces can be sensed as far as the attachment of the periodontal ligament to the cementum. Perhaps the simplest example of clinical observation is the assignment of dental age or the assessment of dental development by looking into a child’s mouth to note the teeth that have emerged through the gingiva. In the absence of other data, however, the number of teeth present are simply counted.1
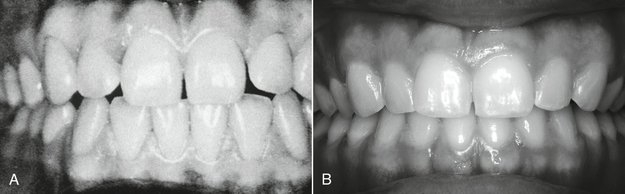
When observations from clinical and radiographic sources of information are coupled with sufficient knowledge of dental morphology and the chronologies of the human dentition, the clinician has the foundation for the diagnosis and management of most disorders involving the size, shape, number, arrangement, esthetics, and development of the teeth and also problems related to the sequence of tooth eruption and occlusal relationships. For example, in Figure 2-1, A, the gingival tissues are excellent; however, the form of the maxillary incisors and interdental spacing might be considered to be an esthetic problem by a patient. To accept the patient’s concern that a cosmetic problem is present and needs correction requires that the practitioner be able to transform the patient’s idea of esthetics into reality by orthodontics and cosmetic restorative dentistry. The situation in Figure 2-1, B demonstrates a periodontal problem (localized gingivitis of the gingival margin of the right central incisor), which is in part a result of the inadequate proximal contact relations of the incisors, leading to food impaction and accumulation of dental plaque and some calculus. For the most part, however, it is the result of inadequate home care hygiene. Most conservative correction relates to removal of the irritants and daily tooth brushing and dental flossing, especially of the interproximal areas of the central incisors. Even so, the risk factor of the inadequate proximal contact remains. If the form of a tooth is not consistent with its functions in the dental arches, then it is highly probable that nonfunctional positions of interproximal contacts will lead to the problems indicated in Figure 2-1, B.
Variability
Uncommon variations in the maxillary central incisors, which are shown in Chapter 6 (see Figure 6-12), reflect samples drawn from a population made up largely of EAa. It is possible to accept the incisors shown as being representative of this population, or perhaps “normal” for the EAa population at the time sampled. A shovel-shaped incisor trait is found in a Caucasoid population only infrequently (fewer than 5%); however, it is one of the characteristics found in patients with Down syndrome (trisomy 21) and normally in Chinese and Japanese individuals, Mongolians, and Eskimos. Statistically then, the shovel-shaped trait might be considered to be abnormal in the Caucasoid population but not so in the Mongoloid populations. The practitioner must be prepared to adjust to such morphological variations.
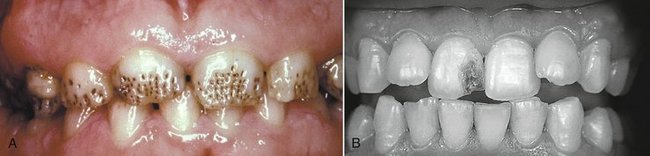
Malformations
Patients who have a disturbance such as the ones shown in Figure 2-2 not only want to know what to do about it, they want to know when or how the problem might have happened. How the problem came about is the most difficult part of the question. Enamel hypoplasia is a general term referring to all quantitative defects of enamel thickness. They range from single or multiple pits to small furrows and wide troughs to entirely missing enamel. Hypocalcification and opacities are qualitative defects. The location of defects on tooth crowns provides basic evidence for estimating the time of the development of the defect with an unknown error and potential bias.2–5 One method of estimating is provided in the section on Tooth Formation Standards in this chapter.
In a cleft palate and lip, various associated malformation of the crowns of the teeth of both dentitions occurs. The coronal malformations are not limited to the region of the cleft but involve posterior teeth as well.6 A number of congenital malformations involving the teeth are evident, with some the result of endogenous factors and others the result of exogenous agents. When a malformation has some particular characteristics (e.g., screwdriver-shaped central incisors) and is consistent with a particular phase of dental development, it may be possible to determine the cause of the disturbance. This aspect is considered further in the section on Dental Age in this chapter.
Chronology of Primary Dentition
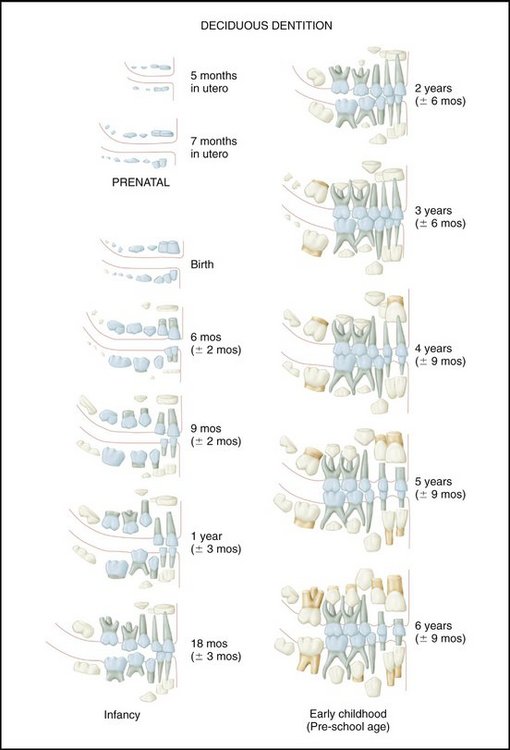
The chronology of the primary teeth presented in Table 2-1 is based on data derived from Tables 2-3 and 2-4 in the section on Tooth Formation Standards in this chapter. The universal numbering system is used in Table 2-1. The pictorial charts (Figures 2-3 and 2-4) are not intended to be used as ideal standards of normal development. Their use is directed toward showing patients the general aspects of development rather than providing precise guidance for clinical procedures.

Development and Eruption/Emergence of the Teeth
Historically, the term eruption was used to denote the tooth’s emergence through the gingiva, but then it became more completely defined to mean continuous tooth movement from the dental bud to occlusal contact.7 Not all tables of dental chronologies reflect the latter definition of eruption, however; the terms eruption and emergence are used here at this time in such a way as to avoid any confusion between the historical use of eruption and its more recent expanded meaning.
Emergence of the primary dentition takes place between the sixth and thirtieth months of postnatal life. It takes from 2 to 3 years for the primary dentition to be completed, beginning with the initial calcification of the primary central incisor to the completion of the roots of the primary second molar (see Figure 2-3).
The emergence of the primary dentition through the alveolar mucous membrane is an important time for the development of oral motor behavior and the acquisition of masticator skills.8 At this time of development, the presence of “teething” problems suggests how the primary dentition can affect the development of future neurobehavioral mechanisms, including jaw movements and mastication. Learning of mastication may be highly dependent on the stage and development of the dentition (e.g., type and number of teeth present and occlusal relations), the maturation of the neuromuscular system, and such factors as diet.
PRIMARY TEETH
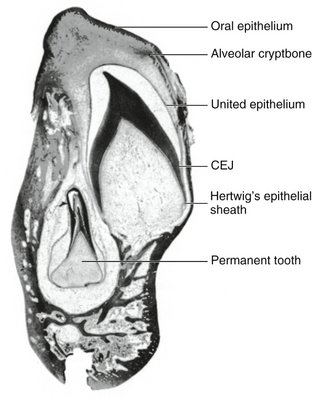
Enamel organs (Figure 2-5) do not all develop at the same rate; some teeth are completed before others are formed, which results in different times of eruption for different groups of teeth. Some of the primary/deciduous teeth are undergoing resorption while the roots of others are still forming. Not all the primary teeth are lost at the same time; some (e.g., central incisors) are lost 6 years before the primary canines. Groups of teeth develop at specific rates so that the sequence of eruption and emergence of the primary/deciduous teeth is well defined with few deviations. Even so, for the individual child, considerable variation in the times of emergence of the primary dentition may occur. The primary dentition is completely formed by about age 3 and functions for a relatively short period of time before it is lost completely at about age 11. Permanent dentition is completed by about age 25 if the third molars are included (see Figures 2-3 and 2-4).9
Calcification of the primary teeth begins in utero from 13 to 16 weeks postfertilization. By 18 to 20 weeks, all the primary teeth have begun to calcify. Primary tooth crown formation takes only some 2 to 3 years from initial calcification to root completion. However, mineralization of the permanent dentition is entirely postnatal, and the formation of each tooth takes about 8 to 12 years. The variability in tooth development is similar to that for eruption, sexual maturity, and other similar growth indicators.10
Crown and Root Development
Dental development can be considered to have two components: (1) the formation of crowns and roots and (2) the eruption of the teeth. Of these two, the former seems to be much more resistant to environmental influences; the latter can be affected by caries and tooth loss.11,12
The Dentitions
PRENATAL/PERINATAL/POSTNATAL DEVELOPMENT
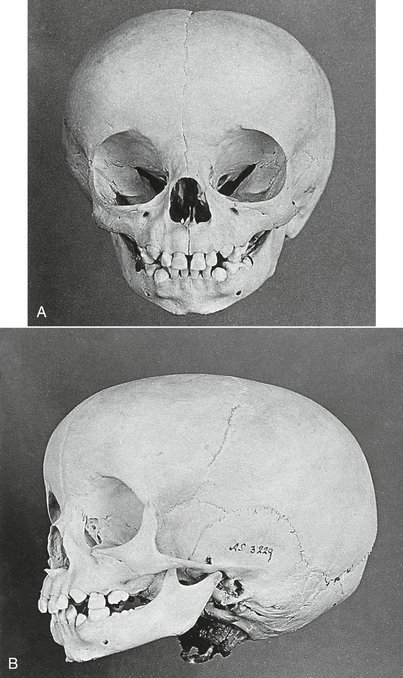
The first indication of tooth formation occurs as early as the sixth week of prenatal life when the jaws have assumed their initial shape; however, at this time the jaws are rather small compared with the large brain case and orbits. The lower face height is small compared with the neurocranium (Figure 2-6). The mandibular arch is larger than the maxillary arch, and the vertical dimensions of the jaws are but little developed. When the jaws close at this stage in the development of the dentition, they make contact with the tongue, which in turn makes contact with the cheeks. The shape of the prenatal head varies considerably, but the relative difference between the brain case, orbits, and lower face height remains the same. All stages of tooth formation fill both jaws during this stage of development.

SEQUENCE OF EMERGENCE OF PRIMARY TEETH
The predominant sequence of eruption of the primary teeth in the individual jaw is central incisor (A), lateral incisor (B), first molar (D), canine (C), and second molar (E), as seen in Table 2-1. Variations in that order may be the result of reversals of central and lateral incisors or first molar and lateral incisor, or eruption of two teeth at the same time.13 This subject is considered in more detail in the section on Tooth Formation Standards in this chapter and in Chapter 16, which addresses development of the primary occlusion.
Investigations of the chronology of emergence of primary teeth in different racial and ethnic groups show considerable variation,7 and little information is available on tooth formation in populations of nonwhite/non-European ancestry.14 World population differences in tooth standards suggest that patterned differences may exist that in fact are not large.14 Tooth size, morphology, and formation are highly inheritable characteristics.15 Few definitive correlations exist between primary tooth emergence and other physiological parameters such as skeletal maturation, size, and sex.16
EMERGENCE OF THE PRIMARY TEETH
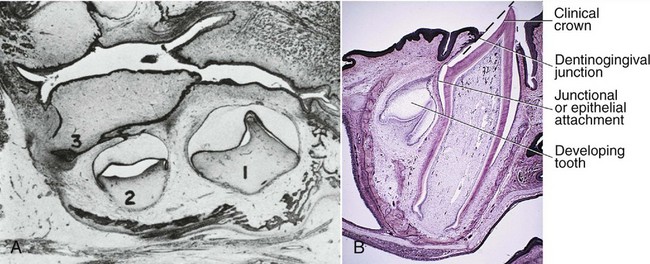
At about 8 (6 to 10) months of age, the mandibular central incisors emerge through the alveolar gingiva, followed by the other anterior teeth, so that by about 13 to 16 months, all eight primary incisors have erupted (see Table 2-1). Then the first primary molars emerge by about 16 months of age and make contact with opposing teeth several months later, before the canines have fully erupted. Passage through the alveolar crest (Figure 2-7) occurs when approximately two thirds of the root is formed,17 followed by emergences through the alveolar gingiva into the oral cavity when about three fourths of the root is completed.18 The emergence data are consistent with those of Smith.14
The primary first molars emerge with the maxillary molar tending most often to erupt earlier than the mandibular first molar.19 Some evidence shows a difference by gender for the first primary molars, but no answer is available for why the first molar has a different pattern of sexual dimorphism.7
The primary maxillary canines erupt at about 19 (16 to 22) months (Figure 2-8), and the mandibular canines erupt at 20 (17 to 23) months. The primary second mandibular molar erupts at a mean age of 27 (23 to 31, boys) (24 to 30, girls) months, and the primary maxillary second molar follows at a mean age of 29 (25 to 33 ± 1SD) months. In Figures 2-8, A and B, the first molars are in occlusion.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


