Traumatic Dental Injuries: Follow‐Up and Long‐Term Prognosis
Eva Fejerskov Lauridsen, Simon Storgård Jensen, and Jens O. Andreasen
Long‐term prognosis after traumatic dental injury mainly depends on the type and extent of injury, correct initial treatment, and systematic clinical and radiographic follow‐up that allows early identification and appropriate handling of potential healing complications.
A traumatic dental injury represents acute transmission of energy to the tooth and supporting structures, which can result in fracture and/or displacement of the tooth, separation or crushing of the supporting tissues [gingiva, periodontal ligament (PDL), and bone] and damage to the neurovascular supply to the pulp. A variety of healing complications may occur after traumatic dental injury. The type and severity of complications depend upon the tissues involved.
Wound healing events
Wound healing events comprise revascularization of ischemic tissue or formation of new tissue in the case of tissue loss (Figure 19.1). In both instances, wound healing takes place by a coordinated migration of cells into the traumatized area, where macrophages form the healing front, followed by endothelial cells and fibroblasts. Vascular loops are formed in a stroma of tissue dominated by immature collagen (Type III) and proliferating fibroblasts. These cells are synchronized via chemical signals released by the involved cells and the surrounding tissue. This phenomenon has been termed the wound healing module [1].
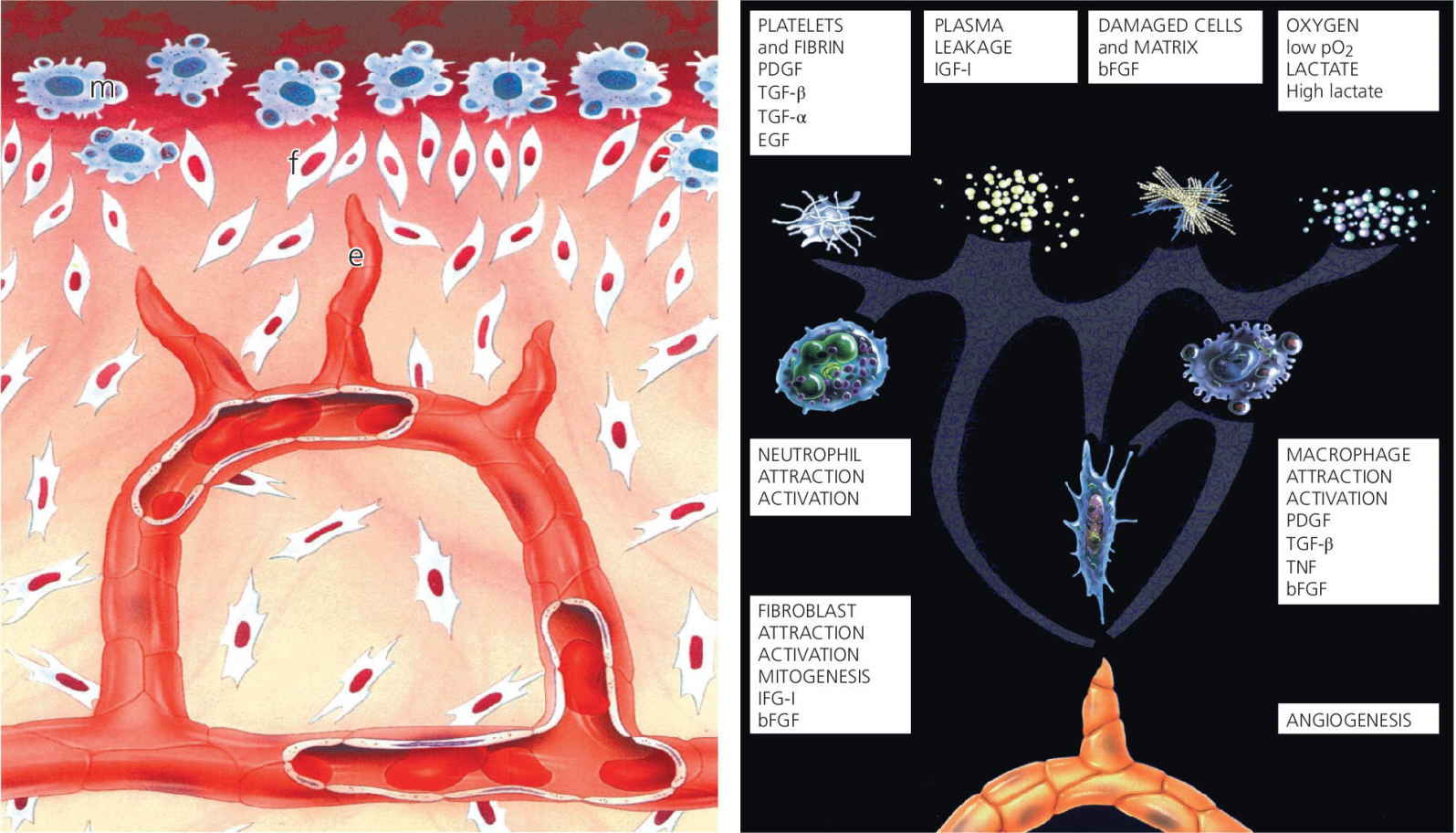
Figure 19.1 Later wound healing events; macrophages (m) form the healing front, followed by endothelial cells (e) and fibroblasts (f).
Source: Andreasen 1995 [9]. Reproduced with permission of F. Andreasen.
In the following, wound healing responses will be described as they appear in the case of simple luxation injuries, with only a separation injury of the PDL and the pulp, and subsequently with more complicated luxation trauma accompanied by crushing injuries [2] (Figures 19.2 and 19.3).
- Separation injuries (Figure 19.2). In the case of separation injury (e.g., extrusive luxation), the major part of the injury consists of cleavage of intercellular structures (collagen and intercellular substance), while there is limited damage to the cells in the traumatized area. This implies that wound healing can occur from existing cellular systems with a minimum of delay [2]. After 1 week, new collagen formation starts to unite the severed PDL fibers which results in initial consolidation of a luxated or a replanted tooth. After 2 weeks, repair of the principal fibers is advanced to a degree where approximately two‐thirds of the mechanical strength of the PDL is regained. In luxated teeth with a severed vascular supply, ingrowth of new vessels into the pulp starts 4 days after injury and proceeds at a speed of approximately 0.5 mm per day in teeth with open apices. Revascularization is usually markedly influenced by the size of the pulpo‐periodontal interface, being almost complete and predictable in teeth with open apices (≥1.0 mm). The chance of revascularization is decreasing with the diameter of the apical foramen and becomes rare with an apical foramen of <0.5 mm [2].
- Crushing injury (Figure 19.3). In complicated luxation injuries with crushing (e.g., intrusion) or other damage of the PDL (e.g., dissection after avulsion), there is extensive damage to both cellular and intercellular systems; and damaged tissue must be removed by macrophages and/or osteoclasts before the traumatized tissue can be restored. Such damage adds several weeks to the healing process. If the protecting cementoblast layer and the epithelial rests of Malassez along the root surface have been destroyed due to the trauma, there is free access for osteoclasts and macrophages to remove damaged PDL and cementum on the root surface leading to root resorption [2].
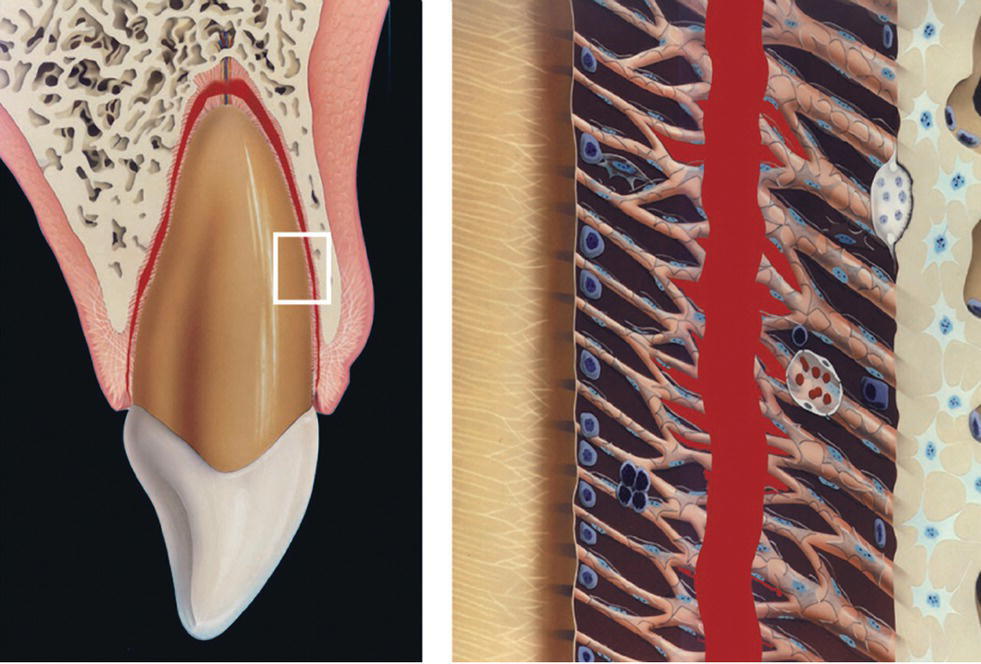
Figure 19.2 Nature of trauma in the case of separation injury.
Source: Andreasen 1995 [9]. Reproduced with permission of F. Andeasen.
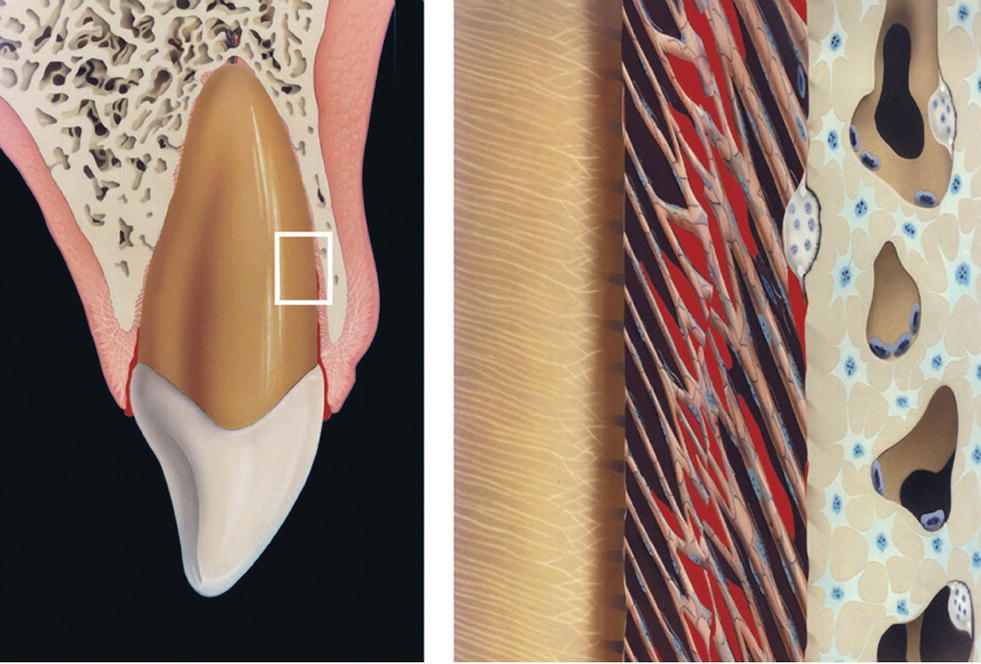
Figure 19.3 Nature of trauma in the case of crushing injury.
Source: Andreasen 1995 [9]. Reproduced with permission of F. Andreasen.
To ascertain the progress of healing and/or the initiation of complications, detailed clinical and radiographic examination must be carried out at specific intervals where complications have become diagnosable.
Primary teeth: follow‐up and prognosis
If it is decided to preserve a traumatized primary tooth, it should be carefully observed for clinical and radiographic signs of pulpal or periodontal complications. Radiographs must also be examined closely to disclose any damage to the permanent successor (Figure 19.4). The patient should always be evaluated one week after the injury to assure initial healing has taken place. Thereafter the intervals between re‐examinations will depend on the type of injury, the expected type of complication and the age of the child. Hence, if there is a low risk of healing complications (e.g., concussion, subluxation or enamel–dentin fracture) and good parental support, then it may be sufficient to evaluate the traumatized teeth once a year. However, parents must then be carefully instructed to contact the dentist if there is any sign of infection such as discoloration of the crown, swelling or pain. In severe cases where there is a high risk of complications (e.g., intrusions or lateral luxation) it is recommended to see the child after 1 week, 4 weeks, 3 months, 6 months, and 1 year, and then annually until the primary tooth is shed and the permanent successor is in place.
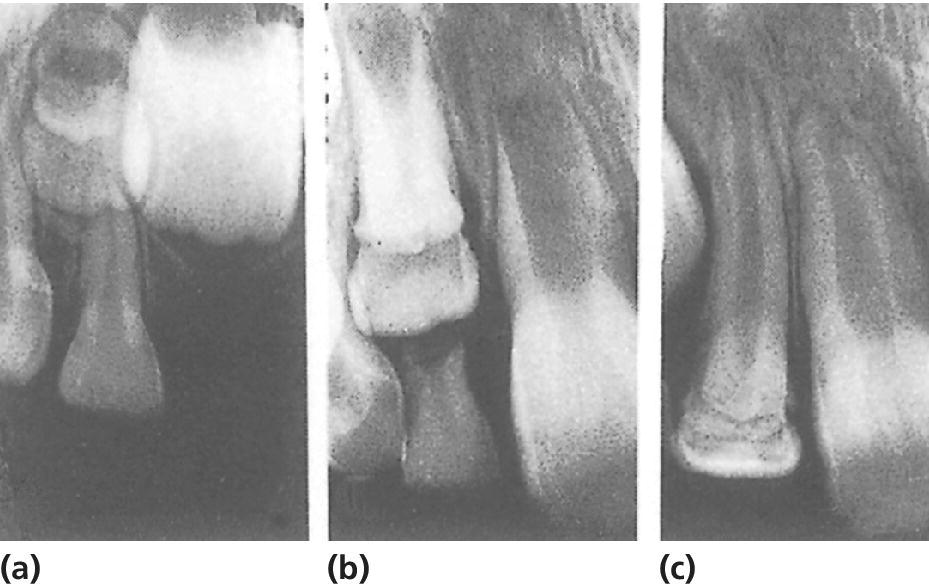
Figure 19.4 Severe malformation of permanent lateral incisor following intrusive luxation of predecessor at the age of 2 years. (a) Condition 1 year after trauma. (b,c) Further development of deformed incisor and uncomplicated eruption, respectively.
Pulpal and periodontal complications
Pulp necrosis
Pulp necrosis is the most common complication [3]. In evaluating pulpal status in primary teeth, sensitivity testing is of limited value, due to the difficulty in obtaining adequate cooperation from the child. Most often, diagnosis of necrosis is based on inspection of tooth color, response to percussion testing, radiographic observation of a periapical lesion or the presence of a fistula or abscess in relation to the traumatized tooth.
Discoloration of the tooth crown is an important sign of the condition of the pulp. It is observed that traumatized teeth with a normal color only rarely develop periapical inflammation. A discolored tooth, on the other hand, is not necessarily indicating the necrotic state of the pulp. A grayish discoloration recorded shortly after a trauma frequently reflects intrapulpal bleeding. On further examination, the gray hue may gradually fade, and return to normal or almost normal. In this case, the pulp will retain its vitality. However, if the grayish color persists, necrosis should be suspected. Information on the pulpal condition can also be obtained by evaluation of the size of the pulp cavity. If pulp necrosis has occurred, normal physiologic reduction in size will not take place. At the first sign of infection, i.e., formation of a periapical radiolucency (Figure 19.5), fistula or abscess formation, extraction is the treatment of choice to prevent possible sequelae to the permanent successor [4].
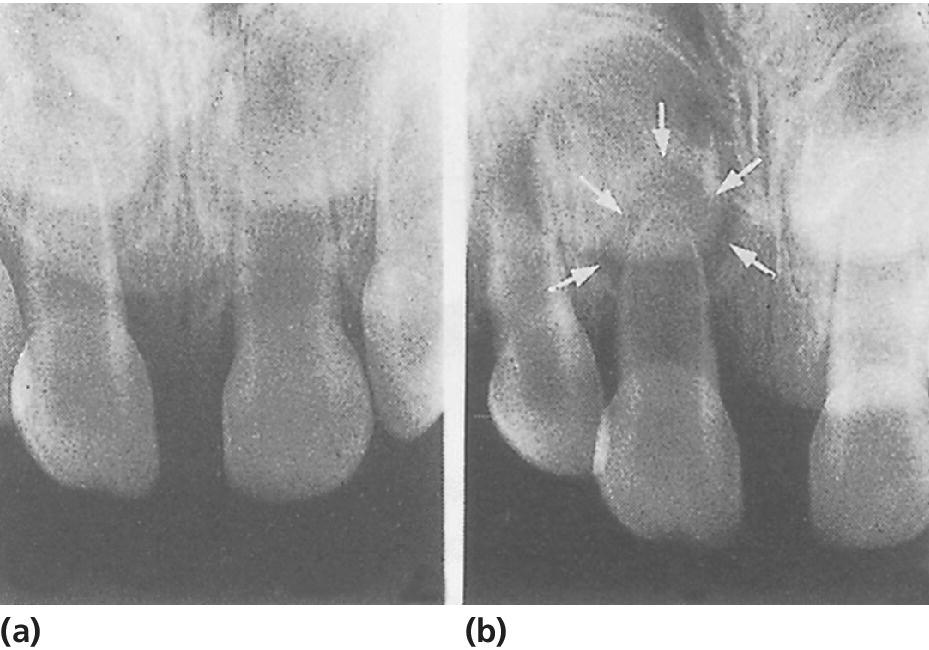
Figure 19.5 (a) Radiograph taken 1 week after slight intrusive luxation of right central incisor. (b) Three months after the trauma there is marked periapical inflammation (arrows).
Pulp canal obliteration
Obliteration of the pulp chamber and canal is a frequent reaction to trauma [3]. The radiograph reveals either partial or total mineralization of the pulp cavity (Figure 19.6). Clinically, the tooth crown gradually assumes a yellowish hue. In the majority of cases, obliterated teeth remain unaffected up to the time of shedding [4].
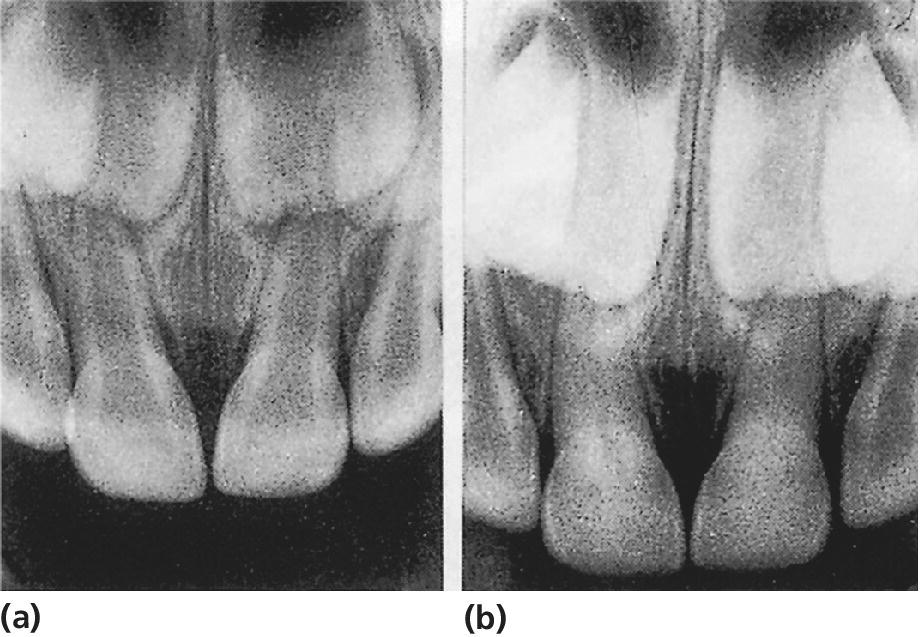
Figure 19.6 Subluxation of both central incisors leading to pulp canal obliteration. (a) At time of injury. (b) Two years later, there is almost total obliteration of the pulps.
Root resorption
The etiology and pathogenesis of root resorption in primary teeth are identical to root resorption in traumatized permanent incisors. External infection‐related root resorption is usually seen after intrusive luxation, whereas internal resorption may develop as a result of both subluxation and luxation injuries [3]. Extraction is the treatment of choice with all types of pathologic root resorption [4].
Injuries to developing permanent teeth
It is well documented that trauma to a primary tooth is easily transmitted to its permanent successor [5,6]. The highest frequencies of developmental disturbances are found after intrusions, avulsions, and alveolar fractures. Most disturbances occur when the apex of the primary tooth directly traumatizes the permanent tooth bud (Figure 19.7). However, periapical inflammation of the primary tooth may also have harmful effects. The type and severity of disturbances found among permanent incisors are also closely related to the age at the time of injury. A tooth germ is especially vulnerable during its early developmental stages. Thus, the most serious disturbances are seen when the damage occurs before the age of 2 years. Changes in morphology or mineralization of the crown of the permanent incisor are the most common types of complications. These lesions range from small enamel opacities to severe malformations [5,6]. Small enamel opacities on the buccal surface of the incisors is the most frequent sequelae. This type of defect will occur in a case of disturbed enamel maturation in a localized area of the crown. If the ameloblasts are affected during an earlier stage it may result in localized yellow‐brown discoloration and hypoplasia of the enamel (Figures 19.8, 19.9, and 19.10). In case of displacement of a primary tooth directly into the follicle of the permanent successor, dislocation of the mineralized part of the tooth may occur in relation to the soft part of the tooth germ whereby a crown dilaceration will occur (Figure 19.4). A permanent incisor with malformation of the crown has a high risk of pulp necrosis because bacteria can gain access to the pulp through microscopic defects in enamel and dentin. It is therefore recommended to seal the enamel shortly after eruption of the tooth [7]. Trauma may also interfere with root formation, leading to bending of the root or partial arrest of the development [5,6]. Severe malformations of the permanent incisors have been reported in less than 5% of the patients [7]. In these cases it is recommended to monitor the patients closely around the time of eruption. The malformed tooth may fail to erupt due to the damage that has been inflicted on the dental follicle. It can be important to preserve a malformed incisor, in order to secure a normal development of the alveolar bone in the region.
Figure 19.7 Disturbance of development of permanent tooth bud due to intrusion of primary incisor. Due to laceration of the follicle, disturbances in enamel formation will develop.
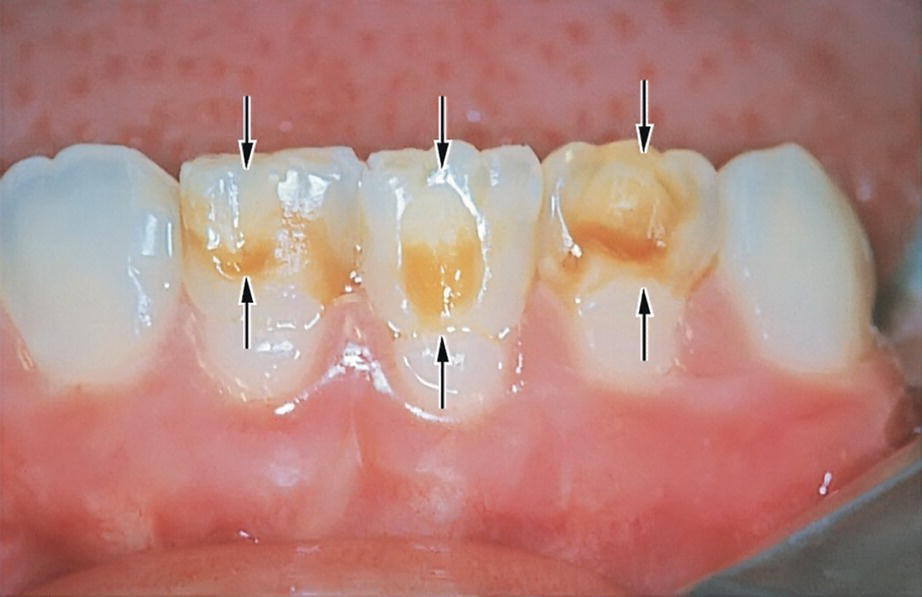
Figure 19.8 Enamel defects in three mandibular incisors (arrows) resulting from avulsion of corresponding predecessors at the age of 2 years.

Figure 19.9 External enamel hypoplasia of right central incisor caused by intrusion of predecessor at the age of 18 months. The hypoplastic area is covered with composite.
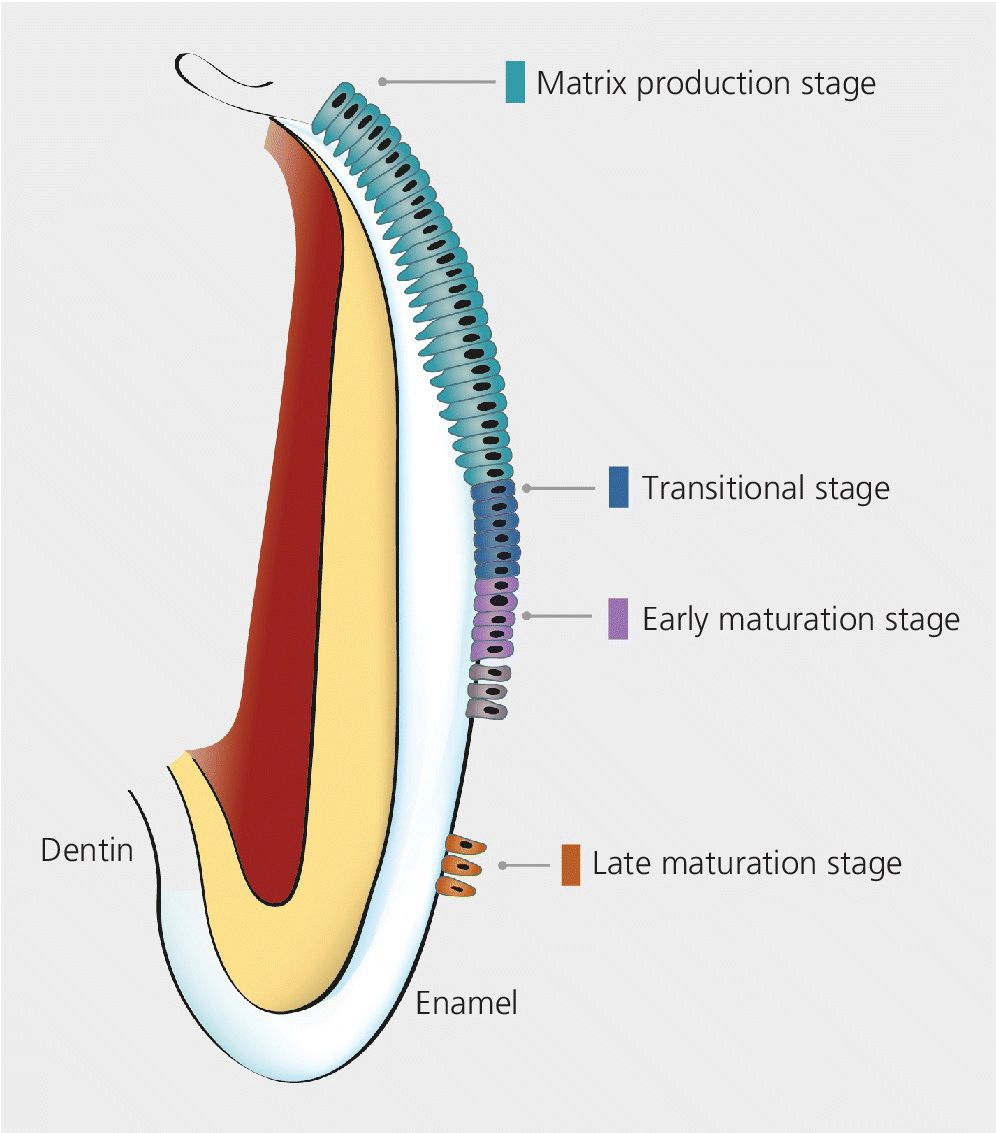
Figure 19.10 A simplified model of the different stages of amelogenesis. The secretory stage where the ameloblasts are secreting the enamel matrix and the early and late maturation fases where the enamel crystals are growing and the mineral content reaches 96% prior to tooth eruption. The reduced enamel epithelium is fusing with the oral epithelium when the tooth is erupting.
Source: Lauridsen et al. 2014 [7]. Reproduced with permission of Danish Dental Journal.
Permanent teeth: follow‐up and prognosis
Due to the variability of dental tissue involved, each specific traumatic injury has an individual prognosis (www.dentaltraumaguide.org). Trauma patients should therefore be recalled with intervals that allow timely diagnosis and treatment of potential complications. Re‐examinations should thus be individualized. Most complications are observed within the first year after trauma. However, the follow‐up evaluation of permanent teeth should continue until treatment of all complications is completed, or until a lost or extracted permanent tooth has been adequately replaced. The following time schedule may serve as a guide for trauma types with moderate or high frequencies of complications: 1 week, 3 weeks, 6 to 8 weeks, 3, 6, and 12 months; thereafter, once a year for 5 years.
The follow‐up examinations should include testing of pulp sensibility, percussion and mobility, and inspection of the tooth color.
A standardized radiographic technique should be used, whereby the tooth is visualized in several projection angles, which are identical during the follow‐up period [8]. The use of film holders is highly recommended.
Pulpal and periodontal complications
Pulp canal obliteration
Pulp canal obliteration is the term used to describe the progressive hard tissue formation within the pulp cavity. A gradual narrowing of the pulp chamber and root canal is observed on radiographs, leading to either partial or total obliteration (Figures 19.11, 19.12, and 19.13). Reduced electrometric response and even loss of sensibility may be recorded as a result of the mineralization. Another clinical observation is a yellowish color of the crown.
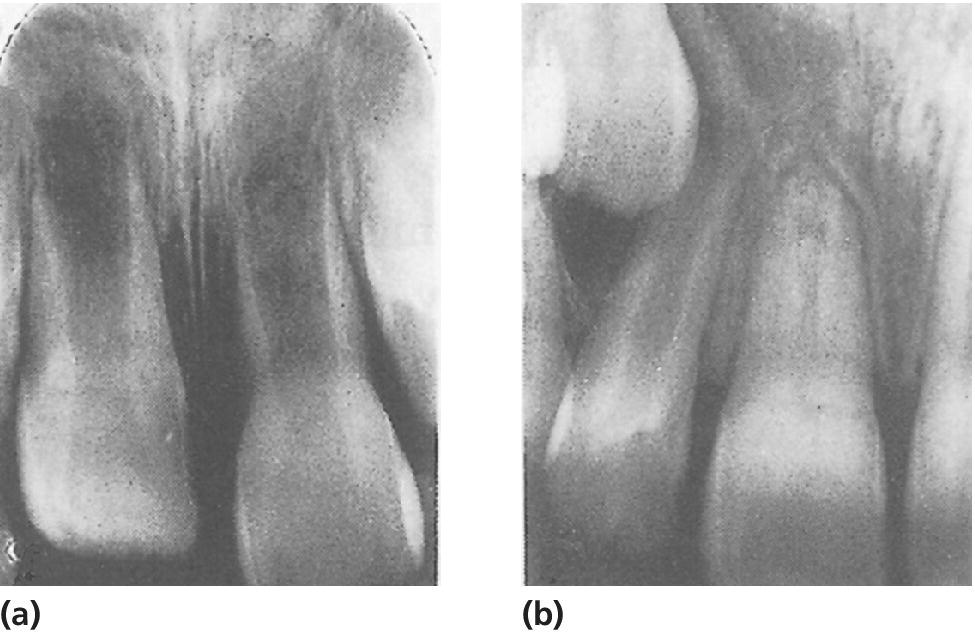
Figure 19.11 (a) Intrusive luxation of immature right central incisor. (b) Spontaneous re‐eruption, closure of apical foramen, and pulp canal obliteration have occurred.
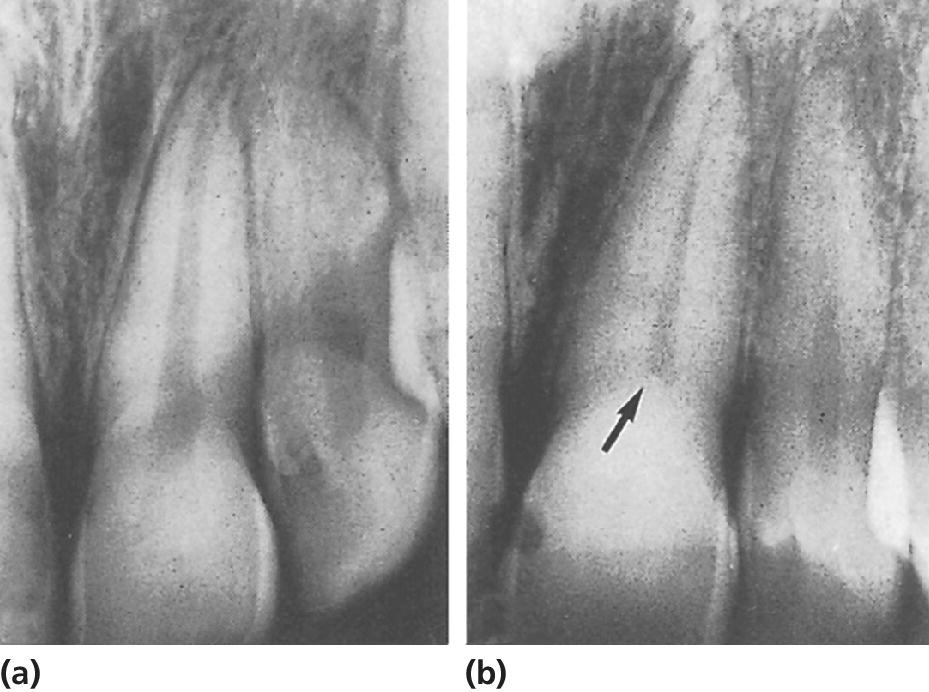
Figure 19.12 Partial pulp canal obliteration in left central incisor. (a) At time of injury. (b) Condition 15 years later. Pulp chamber completely obliterated and root canal slightly reduced in size (arrow).
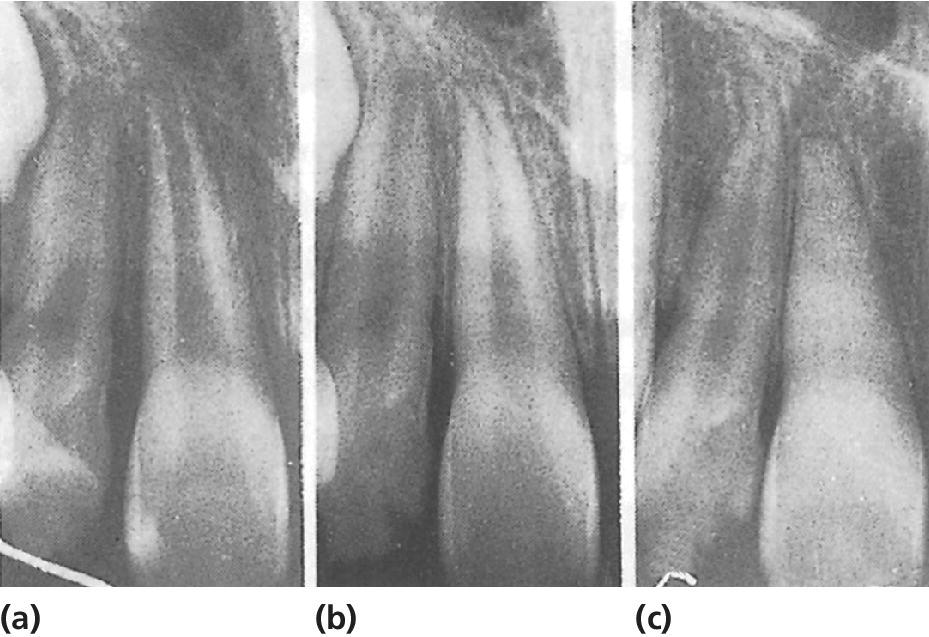
Figure 19.13 Obliteration after successful replantation of right central incisor. The tooth was replanted within a few minutes. (a) Normal findings 3 weeks later. (b) A radiograph taken 6 months later shows apical closure. (c) Seven years after replantation, there is total pulp canal obliteration and no sign of root resorption.
It is not fully understood what stimulates odontoblasts to start the formation of hard tissue on the root canal walls. However, obliteration appears to be significantly related to teeth with incomplete root formation. Obliteration is also more frequent after extrusion, lateral luxation, and intrusion than after concussion and subluxation, which indicates that the disturbance in dentin formation may be related to the revascularization of the pulp [9,10].
Although a radiograph gives the illusion of complete mineralization of the pulp cavity, a minute strand of pulp tissue always remains. In about 13% of these teeth the pulp becomes necrotic and periapical inflammation develops [11,12]. This is a late complication, usually seen 5–20 years after the injury. In a long‐term follow‐up study these pulp necrosis events were found to increase at about 1% per year [13]. Despite the excessive mineralization, the root canal is nearly always accessible for conventional endodontic treatment.
Pulp necrosis
Pulp necrosis is the most common post‐traumatic complication [9]. If the neurovascular supply to the pulp is severed at the time of injury, pulp healing may occur due to ingrowth of new blood vessels and nerve fibers. Revascularization of the pulp is most likely to occur in teeth with immature root development; but in children and adolescents it may also occur in teeth with mature root development. However, it is only possible in the absence of bacteria in the root canal. The long‐term prognosis of the pulp is therefore primarily related to the extent of damage to the neurovascular supply (related to the type of luxation), and the possibility of revascularization of the pulp (reflected by the stage of root development) [9]. Bacteria may gain access to the pulp through exposed dentin, e.g., in case of fracture of the crown or damage to the root surface. Hence, teeth with combination injuries (luxation injury and a crown fracture) have an increased risk of pulp necrosis [14–16].
Clinical signs of pulp necrosis
While some pulp necroses can be diagnosed within the first 3 months after injury, years may pass before signs of necrosis become apparent. Diagnosing pulp necrosis usually implies the use of pulp sensibility testing, evaluation of color changes, and radiographic examination for signs of pathosis such as periapical radiolucency, root resorption, and/or arrested root development.
Pulp sensibility testing. Sensibility testing can be performed with an electric pulp test, cold test, or by blowing air on exposed dentin. It is important to bear in mind that it is a measure of the sensory nerve activity and not a measure of the vitality of the pulp. In case of revascularization after complete severance of the pulp, the regeneration of the sensory nerves takes longer than the ingrowth of new blood vessels [2]. The tooth may therefore not respond to sensibility test until 3–12 months after injury. A negative test alone should, therefore, not be regarded as proof of necrosis. Endodontic treatment should always be postponed until at least one other clinical and/or radiographic sign of necrosis appears. In addition, teeth with immature root development may have a higher threshold for reaction to sensibility test because the sensory nerves are not yet fully developed.
Tooth discoloration. An almost immediate pinkish discoloration indicates intrapulpal bleeding caused by the trauma. In the following weeks the red color may turn gray but in case of pulp healing, the discoloration will gradually fade away (Figure 19.14). However, if the tooth crown turns progressively gray, necrosis should be suspected. A grayish color that appears for the first time several weeks or months after trauma is regarded as a sign of necrosis. In this case, the gray color signifies decomposition of necrotic pulp tissue. Teeth with pulp canal obliteration may appear yellow [8].
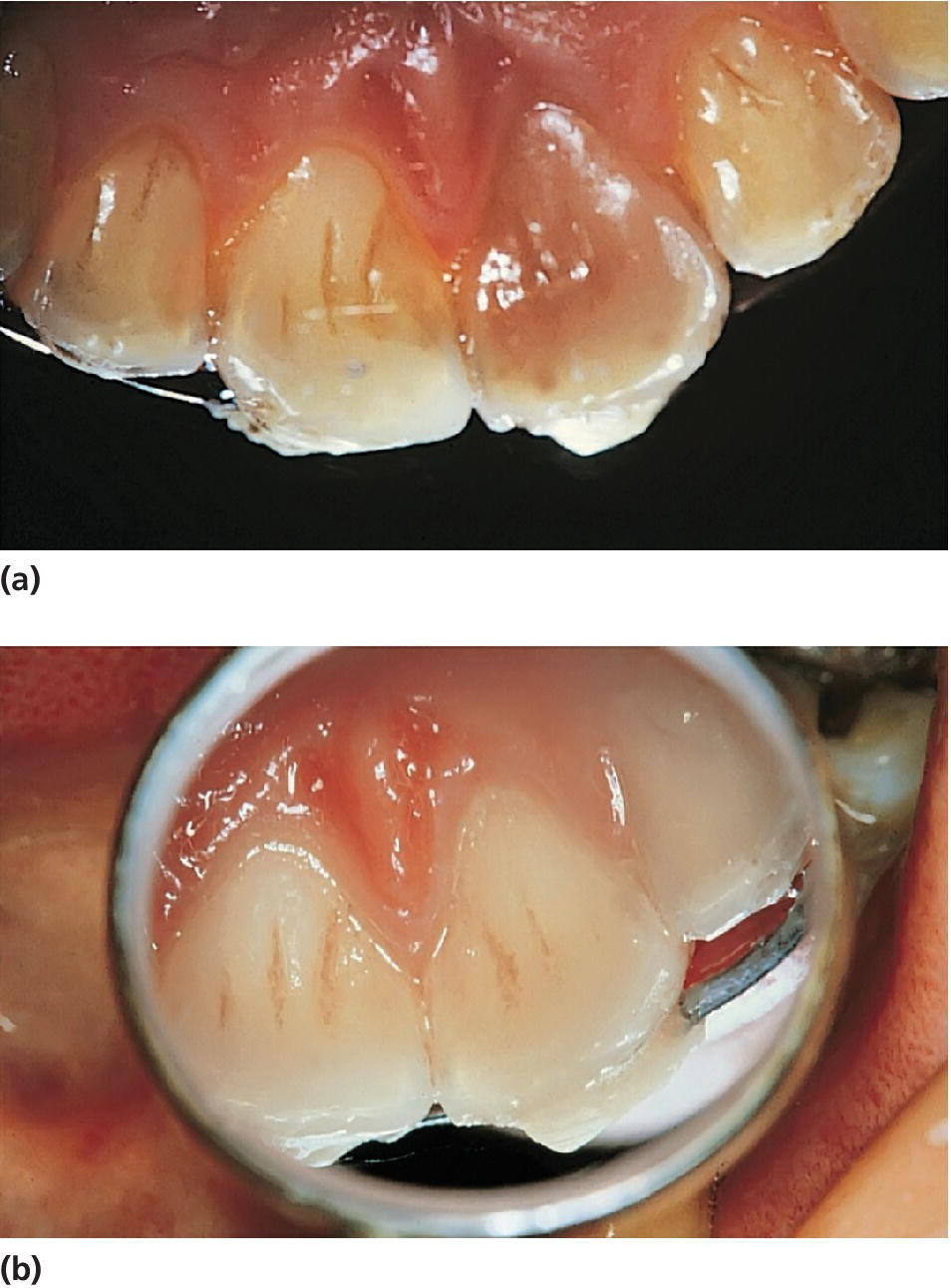
Figure 19.14 (a) Left central incisor in 10‐year‐old boy discolored within 1 week after subluxation injury. (b) Three months later. Discoloration has disappeared and the tooth responds normally to electrometric pulp testing.
Radiographic signs of pulpal necrosis
To get maximum information from a radiographic follow‐up it is mandatory that a standardized radiographic technique is used to ensure that series of radiographs may be adequately compared. The use of filmholders is therefore recommended.
Periapical radiolucency. An increased width of the periodontal ligament and loss of lamina dura in the apical area, may be a sign of pulp healing seen in relation to revascularization of the pulp. However, increasing size of the defect and development of a persistent apical radiolucency indicate periapical inflammation in respond to bacteria in the root canal [8].
Arrest of root development. If necrosis involves the epithelial root sheath before root development is complete, no further root growth takes place. It should be borne in mind that necrosis may progress from the coronal to the apical part of the pulp. In this way, vitality may apparently persist for a while apically, resulting in the formation of a calcified barrier across the wide apical foramen [2] (Figure 19.15).
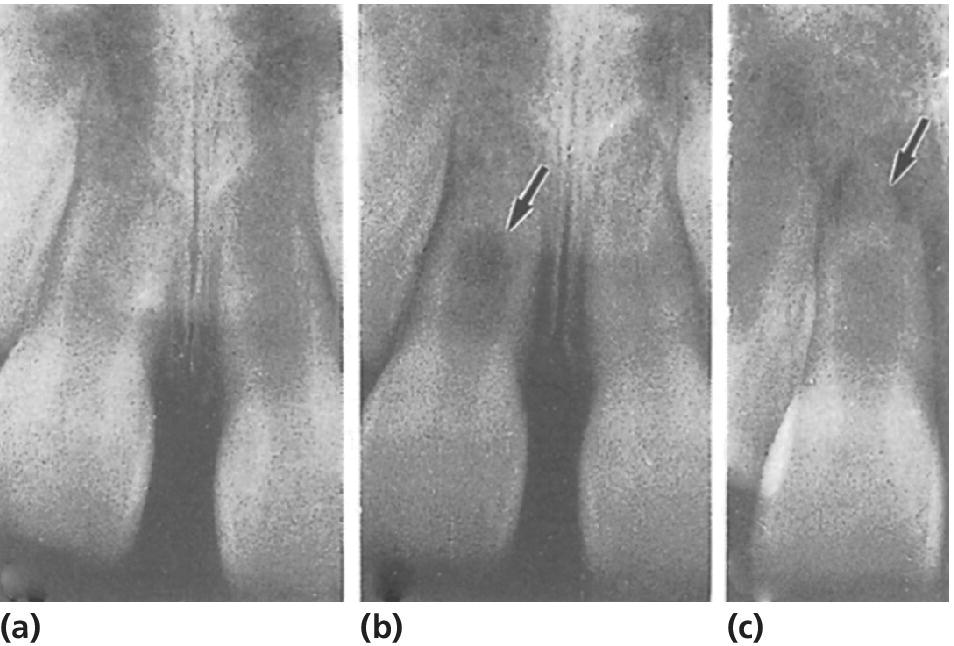
Figure 19.15 Pulp necrosis of right central incisor following intrusion. (a) Re‐eruption took place 3 months after injury. (b) No further root development. Hard tissue formation (arrow) is found together with continued vitality. (c) Pulp necrosis is diagnosed from a periapical radiolucency (arrow), which developed 1 year after injury.
Cervical root fractures after endodontic treatment
Endodontic treatment of nonvital immature teeth is reported to be highly successful (see Chapter 17). However, it is important to realize that success refers to the primary goal: a tight apical seal. Necrosis in a developing tooth results in arrested dentin formation, often resulting in thin dentinal walls. These fragile walls are susceptible to fracture particularly in the cervical area (Figure 19.16). The frequency of cervical root fracture is reported to range from 2% in an 11‐year‐old to 77% in a 6‐year‐old (Box 19.1) [17]. The thin dentinal walls are the main reason for cervical fractures. However, it has been reported that long‐term use of calcium hydroxide for apexification of immature roots increases the risk of these cervical fractures [18]. This finding has led to a shift in the endodontic procedure for teeth with immature root formation, and formation of an apical plug with MTA is therefore now the recommended procedure. However, the prognosis should still be regarded as doubtful to poor with pulp necrosis in children 6–10 years of age, and an alternative long‐term treatment plan should be considered. This is of particular importance in malocclusion cases where extraction of premolars is part of the orthodontic treatment plan. The question is whether a nonvital immature incisor with doubtful prognosis should be kept for as long as possible for later prosthetic replacement, or whether the traumatized tooth should be removed and the space closed orthodontically or by premolar autotransplantation.
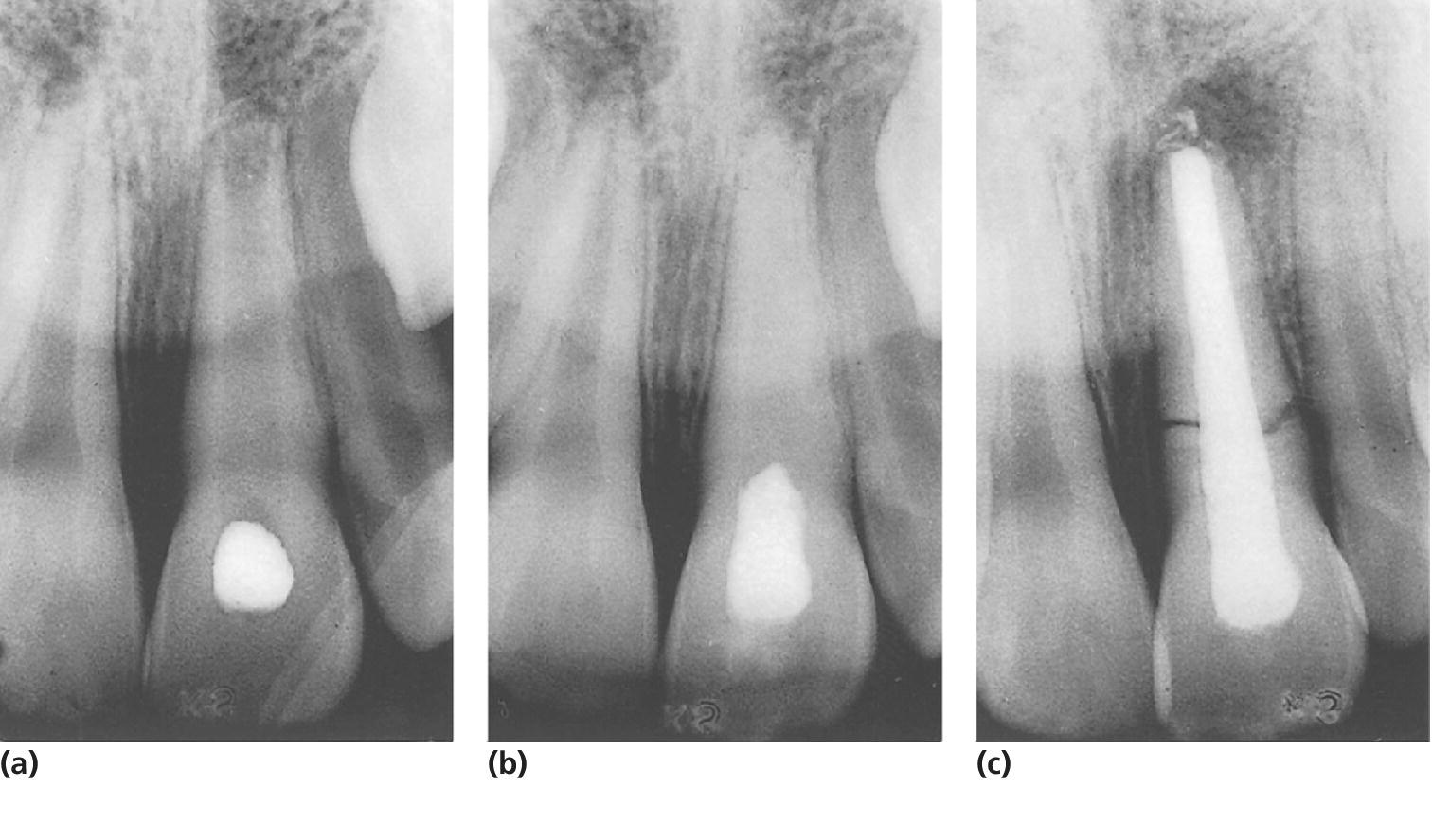
Figure 19.16 Spontaneous root fracture of nonvital immature central incisor. (a, b) During long‐term treatment with calcium hydroxide. (c) The fracture was observed 1 year after completed endodontic treatment.
VIDEdental - Online dental courses


