18
Progressive Slenderizing Technique
Definition and objectives
Anthropological justification of slenderizing
Influence of slenderizing on dental plaque, caries and periodontal disease
Indications
Contraindications
Advantages of slenderizing
How much enamel can be stripped?
Special considerations
Instrument for slenderizing
Progressive slenderizing technique
Clinical procedure
Biomechanical archwire sequence
Case reports
References
Definition and Objectives
Slenderizing refers to the mechanical reduction of the dental interproximal enamel layer, which is carried out in order to re-shape the contact area and decrease the mesiodistal diameter of the teeth to facilitate alignment. Compared with extractions, slenderizing allows removal of only the required amount of tooth material without decreasing the vertical dimension or adversely affecting the profile through retraction of the incisors, and it also avoids other side effects of the space closure.
The ratio between the enamel loss and space gain is 1:1, that is, for each millimetre of slenderizing, 1 mm of space is gained. The orthodontist can maintain anchorage during the treatment, if he or she wants to use this space for achieving the orthodontic objectives.
The objectives of slenderizing include:
- Correction of dentoalveolar discrepancies
- Treatment of tooth size discrepancy between the upper and lower teeth (Bolton discrepancy)
- Adjustment of interdental contact point to the papilla shape
- Increasing the interdental contact surface in order to contribute to better stability of corrected rotations
- Improving the occlusion by allowing the tooth cusps of a dental arch to occlude into the interdental embrasures and grooves of the antagonist teeth
- Correction of asymmetries in order to improve aesthetics.
Ballard (1944) described this technique for the first time in 1944. Other authors have since contributed to its development (Sheridan 1997).
Anthropological Justification of Slenderizing
In 1902 Black published a text on teeth anatomy in which he referred to the natural interproximal abrasion of the teeth as natural slenderizing. Begg (1954) and Murphy (1964) studied occlusions of Aborigines presenting interproximal wear, losing up to 14–15 mm of tooth material during their whole life as a consequence of non-refined diets and the absence of crowding. The studies confirmed that slenderizing was necessary in order to increase stability, and part of an adaptation system, which consists of:
- Passive tooth eruption to compensate for occlusal wear: the tooth erupts until it makes contact with the antagonist, and in that way it maintains the occlusion and vertical dimension
- Spontaneous mesial migration to compensate for interproximal wear: this preserves the interdental contact points
- Formation of the secondary dentine to maintain a constant thickness of hard tissue between the dental pulp and the exterior of the tooth
- Increased density as well as accelerated remineralization of enamel in the more abraded zones.
These defence mechanisms, which do not affect reproductive ability or longevity (Begg 1964), are still evident today but the teeth do not get as worn because they are used only for chewing and the food consistency is much more soft than it was in the Stone Age. These dental mechanisms are similar to hair or nail growth.
Harry Sicher (1953), speaking about the attrition of teeth, said that it is possible that wear of teeth has a positive function, and questioned whether nature sacrifices tooth substance to achieve an increase in function. Peck and Peck (1972) discovered the relation between tooth size, mesiodistal and labiolingual widths of the inferior incisors, and the degree of crowding (PI index). Betteridge (1981) also found a relationship between tooth size and degree of crowding (BI index).
These facts can be considered an anthropological base for the practice of current techniques of slenderizing.
Influence of Slenderizing on Dental Plaque, Caries and Periodontal Disease
A comparison of crowded or rotated teeth with teeth aligned after slenderizing demonstrates that accumulation of the bacterial plaque is reduced and hygiene is facilitated following alignment. As far as the relation between slenderizing and caries is concerned, studies carried out by cariologists (Brudevold et al. 1982; El-Mangoury et al. 1991) reveal that dental grinding provokes a defence reaction that creates the nucleation zones for accelerated remineralization. Within a few minutes, the saliva starts to neutralize affected zones and a remineralization process can be demonstrated 1 hour later. At the beginning, the process is very fast but then it slows down and is completed within 9 months. At the end, the enamel is as resistant to caries as it was prior to slenderizing.
As far as the relation between the slenderizing and periodontal diseases is concerned, periodontal defects should be taken into consideration as a result of the balance between the effect and bacterial plaque accumulated in periodontal pockets, and risk factors of each patient. Tooth shape and the anatomy of the interproximal contact points, among other factors, influence the development of periodontal diseases. When the contact points are correctly established, tooth brushing and self-cleaning becomes easier, thus minimizing the food impaction and at the same time, the contact points protect the interdental papilla. The prevalence of intraosseous defects is minor in aligned teeth with good contact points (Heins and Wieder 1986). Also, Nielsen et al. (1980), Tal (1984) and Heins et al. (1988) highlighted the importance of the interradicular width in the creation of interdental septum defects.
Even if we carry out slenderizing on already aligned teeth, the interdental septum thickness is reduced when closing the spaces but the periodontal status is improved according to Betteridge (1976, 1979). Out of 17 cases of slenderizing, he found that 14 had an improved gingival inflammation index; Boese (1980a,b) did not find any significant difference in the alveolar crest height when comparing radiographs of 40 patients before and after slenderizing. Crain and Sheridan (1990) also did not find any significant differences in the gingival index 3–5 years after the end of the treatment in 151 interproximal surfaces treated with slenderizing. In all these studies, the enamel reduction was no more than 0.5 mm per proximal surface.
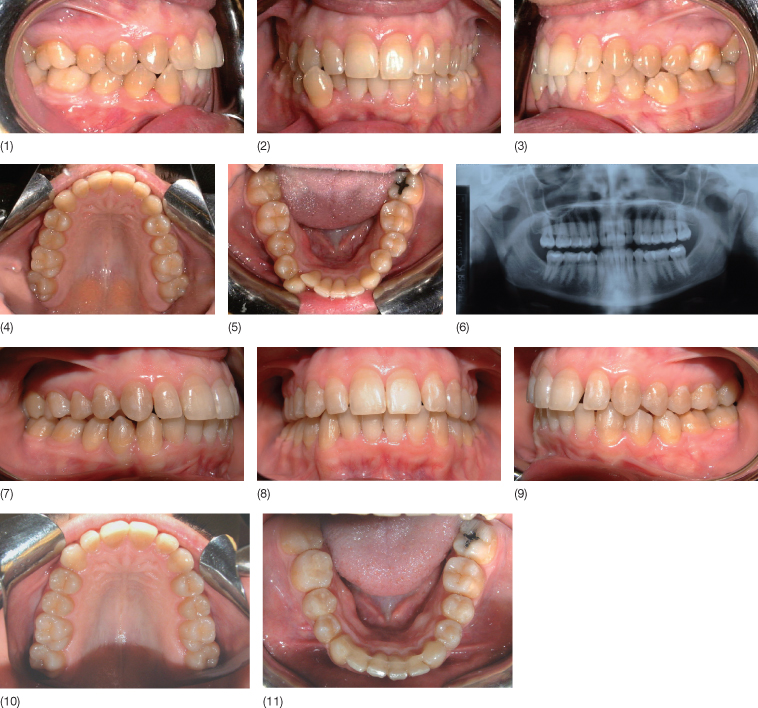
Figure 18.1 presents the case of a 29-year-old female patient with crowding in the lower arch, crossbite of the lower right canine and a midline deviation. She was treated with fixed appliances and slenderizing in the lower arch. The initial panoramic and intraoral views after slenderization and reproximation demonstrate the health of the interdental septum.
Fig. 18.1 (1–5) A 29-year-old female patient with crowding in the lower arch, crossbite of the lower right canine and midline deviation. Intraoral photographs showing the status before treatment. (6) Initial panoramic X-ray. (7–11) Final results. Intraoral X-rays after slenderizing and reproximation: (12) lower right molars; (13) lower right canine; (14) lower incisors; (15) lower left canine; and (16) lower left molars.
Obviously, it is important to avoid gingival injury while carrying out slenderizing. This can be accomplished with brass wire protectors or using Dr Sheridan’s safe tipped burs (Raintree Essix), or Ortho-Strips files (Intensiv), or Orthocare strip files (Dentacare, Swiss Dental). The safe tipped burs have inert tips that do not cause any damage to the gingival tissues, while Orthocare and Ortho-Strips files are made in such a way that they can only cut hard but not soft tissues.
Indications
Crowding
Slenderizing is a technique for the treatment of minor crowding, but an experienced orthodontist also can treat moderate crowding cases.
Bolton Discrepancies
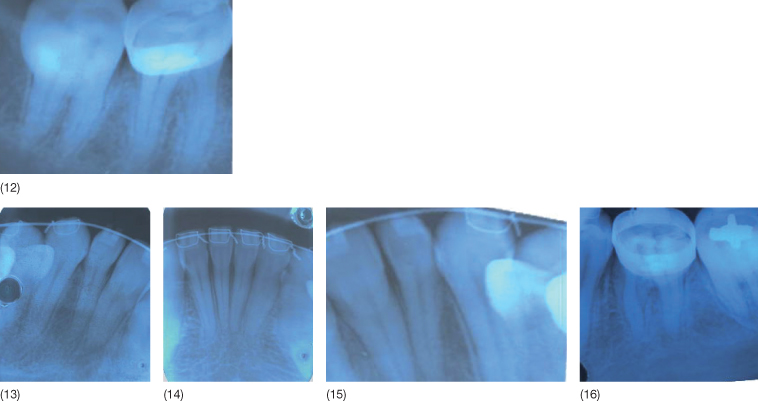
The upper and lower canine-to-canine and upper and lower molar-to-molar Bolton indices indicate where slenderizing might be undertaken to improve the occlusion. Bolton determined that the relation between the upper and lower molar-to-molar tooth size is 91, 3 ± 1.91 (Fig. 18.2) and that the canine-to-canine relation is 77, 2 ± 1.65 (Fig. 18.2). If a ‘12’ Bolton index is achieved, a molar Class I relationship is obtained and if the ‘6’ Bolton index is achieved, a canine Class I relationship is obtained. If the patient presents a Bolton discrepancy, it is necessary to compensate for this discrepancy by slenderizing.
Fig. 18.2 (1) Molar-to-molar Bolton index (12 teeth). (2) Canine-to-canine Bolton index (6 teeth). (3) Tooth shapes according to Bennett and McLaughlin (1997): rectangular, triangular and barrel-shaped teeth.
Triangular and ‘Barrel’ Tooth Shapes
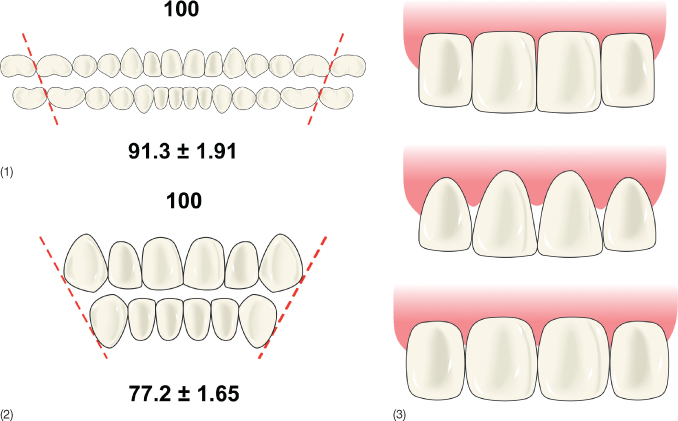
According to Bennett and McLaughlin (1997), we can distinguish three main tooth shapes: rectangular, triangular and a barrel-shaped teeth (Fig. 18.2). Tooth shape has great importance in orthodontic treatment. The rectangular shape allows a wide and stable contact point without visible interdental spaces. The triangular shape allows a reduced and very occlusal or incisal contact point with ‘black gingival triangles’ (Fig. 18.3). Barrel-shaped teeth have a reduced contact point in the middle with apparent embrasures at the incisal level.
Fig. 18.3 (1) Patient with crowding and triangular-shaped teeth. (2) After alignment with lingual brackets, the ‘black gingival triangles’ appeared due to the triangular shape of the teeth. (3) Final result after slenderizing and reproximation (no black gingival triangles).

It is possible that spaces due to triangular or barrel-shaped teeth spaces are not obvious at the beginning of the treatment due to presence of crowding or rotations. The patient in Figure 18.3 had crowding of triangular teeth without interdental spaces. Alignment of the teeth led to development of ‘black gingival triangles’. It is important to inform the patient about this fact before starting the treatment and to include a solution for this problem in the treatment plan. If the dentoalveolar discrepancy is negative, slenderizing and reproximation can solve the problem but if the discrepancy is positive, some aesthetic restorations may be necessary (Fig. 18.4).
Fig. 18.4 (1) Scheme of a case with ‘black gingival triangles’ due to the triangular teeth. (2) Cases with negative dentoalveolar discrepancy are treated with slenderizing and reproximation. (3) Cases with positive dentoalveolar discrepancy are treated with aesthetic restorations.
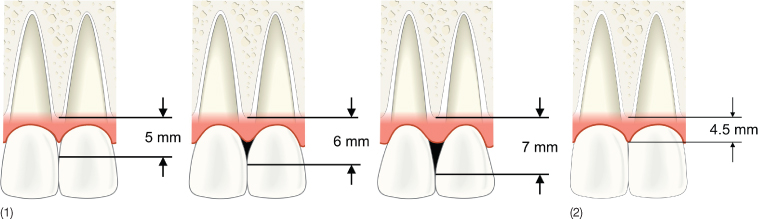
If the crown has a triangular shape, the distance between the bone crest and the contact point is relatively large. In these cases, the interproximal papilla tends to be absent. Tarnow et al. (1992) demonstrated that if the distance from the contact point to the interdental bone crest is 5 mm or less, the papilla is present in 100% of the cases. If this distance is 6 mm, the papilla is found in 56% of the cases and if it is 7 mm or more, the papilla is present only in 27% or less (Fig. 18.5). Therefore he recommended the distance between the bone crest and the top of the papilla should be 4.5 mm (Fig. 18.5).
Fig. 18.5 (1) Tarnow et al. (1992) evaluated the relationship between the distance from the interdental contact point to the bone crest and the presence or absence of ‘black gingival triangles’. (2) The height of the interdental papilla should be 4.5 mm.
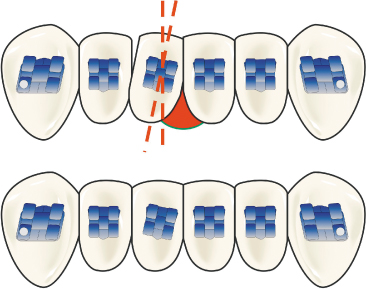
Black gingival triangles do not always appear due to an increase in the distance between the contact point and the bone crest. According to Bennett and McLaughlin (1997) (Fig. 18.6), a black gingival triangle can appear as a consequence of a bracket malpositioning with respect to tooth inclination. In this case, the bracket position should be corrected and slenderizing should not be carried out. In these cases, an ‘occlusal black triangle’ can be observed on the other side of the tooth and the periapical X-ray will show that the roots are not parallel.
Fig. 18.6 Influence of a bracket malposition on inclination and the presence of the ‘black gingival triangles’.
(According to Bennett and McLaughlin 1997).
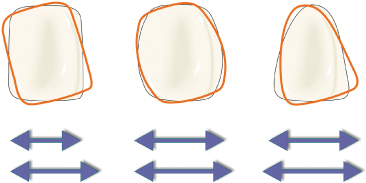
There is no relation between dental shape and the enamel thickness (Fig. 18.7), therefore the amount of possible slenderizing does not depend on the dental shape; however, minimal grinding of triangular and barrel-shaped teeth will generate considerable space in the dental arch. According to Andrews (1989), if the teeth are tipped mesiodistally, they occupy more space in the dental arch than teeth in a more vertical position, but Bennett and Mc Laughlin (1997) emphasize that this fact is more true for rectangular teeth than for other tooth shapes (Fig. 18.8). This is why significant tooth uprighting as a solution for a mild negative discrepancy is possible only in rectangular teeth.
Fig. 18.7 Triangular, ‘barrel-shaped’ and rectangular teeth with different sizes and different thicknesses of the enamel layer.
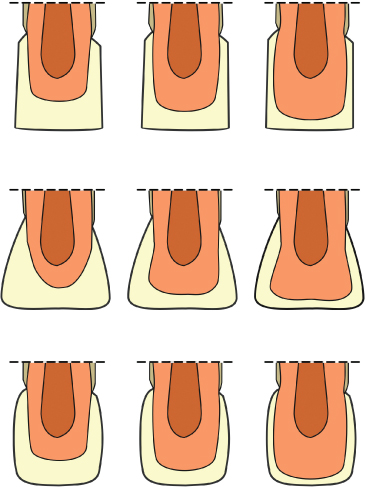
Fig. 18.8 Only the rectangular shape has an important influence on the space occupied by a tooth in the dental arch, in relation to its inclination.
(According to Bennett and McLaughlin 1997).
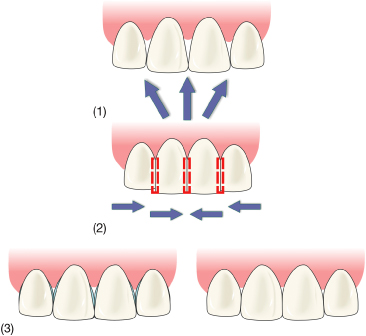
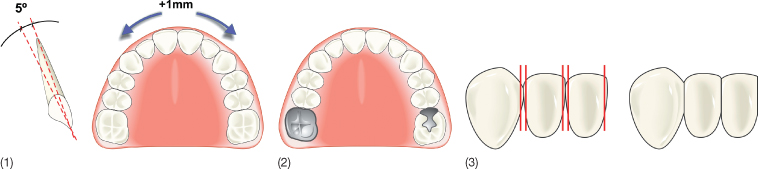
According to Steiner, incisal protrusion allows us to obtain double space, i.e. the discrepancy is reduced by 2 mm for every 1 mm of protrusion. According to Bennett and McLaughlin (1997), increasing the torque without protrusion also permits the orthodontist to gain 1 mm for every 5° of increased palatal root torque (Fig. 18.9).
Fig. 18.9 (1) A 5° torque increase without protrusion allows increase of 1 mm of space in the arch (Bennett and McLaughlin 1997). (2) Over-extended crowns and fillings. (3) With slenderizing and reproximation, the contact point comes closer to the crest of the interdental septum.
(According to Bennett and McLaughlin 1997.)
Macrodontia
Dental shape does not have any influence on the enamel thickness (Fig. 18.7) but it is aesthetically more advisable to perform slenderizing on macrodontic rather than on microdontic teeth. The ‘golden proportion’ described by Ricketts (1989), between upper central incisors and lateral incisors, can serve as a guide.
Over-Extended Crowns and Fillings
In such cases, slenderizing is indicated to obtain normal tooth shape and dimensions (Fig. 18.9).
Bilateral Dental Asymmetries
Slenderizing, veneers or crowns are often indicated in order to compensate for dental asymmetries, especially in the upper anterior region.
Adult Patient (Narrowed Pulp Chambers)
Adults have narrower pulp chambers, so slenderizing can be carried out with less risk of compromising dental sensibility than in young patients.
Low Caries Index
Slenderizing should only be carried out in patients with a low caries index, in order to avoid increase in susceptibility.
Good Oral Hygiene – Low Bacterial Plaque Index
Slenderizing is recommended only in patients with good oral hygiene, in order to avoid the risk of caries.
Multiple Rotations, in Order to Achieve Better Stability
In patients who present with multiple rotations, slenderizing can result in wider interproximal contact areas, which makes the tooth position more stable with respect to the risk of relapse (Fig. 18.9).
Cases Treated with Lower Incisor Extraction
These cases need to be compensated by upper canine-to-canine/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


