Development of Orofacial Complex
• To be aware of the developmental stages of the human from fertilization to birth
• To list the embryonic structures that form the face and discuss the approximate age of formation
• To discuss the mechanism involved in the development of the upper lip
• To name the structures involved in the formation of the palate and the timing of its development
• To describe the mechanism involved in the development of the palate
• To describe the other structures arising from the pharyngeal arches
• To discuss the embryonic structures involved in the development of the cleft lip and palate
PREFACIAL EMBRYOLOGY
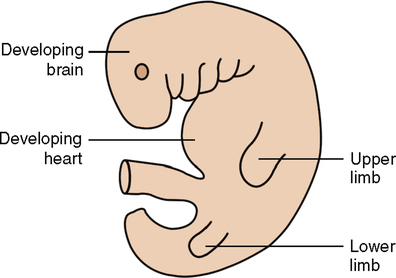
One can begin to see the early features of the face developing by the embryonic age of 3 weeks. By the time the embryo is about 3 weeks old, its length measures approximately 3 to 4 mm from the top of the head to the tail area. Even at that small size, the forerunners of the structures that will become the face can be seen. Fig. 18-1 is a lateral view of the embryo, and several important features can be seen. The umbilical cord (shown cut here) attaches the embryo to the placenta embedded in the wall of the uterus. The heart bulge appears as it does because it develops in an extremely anterior position and pushes out on the upper body wall, which will later become the thorax. As the thorax and ribs develop, the heart will assume a position inside the thoracic cage and will no longer bulge outward. Finally, three ridges of tissue are visible, the pharyngeal arches, which can be seen bulging out laterally. The pharyngeal arches seen in Fig. 18-1 are actually U-shaped bars of tissue. The open end of the U faces posteriorly and surrounds the upper end of the foregut and part of the primitive oral cavity. Eventually six of these arches will develop. The fifth one, however, will degenerate and form nothing of any consequence. The fourth and sixth arches are poorly developed and are not readily seen on the embryonic surface. The ones closest to the head are the largest, and those farther down are smaller in size.
For a better understanding of the structure of these pharyngeal arches, it is necessary to look at a longitudinal section through the embryo, which is divided into equal halves (Fig. 18-2). The body is relatively hollow, with the exception of a tube closed at its upper and lower ends and running through the middle of the body cavity whose lining has developed from entoderm. This tube is the developing digestive tract and is divided into three parts. The upper part is the foregut, which forms the digestive tube from the throat region to the duodenum. The middle portion is the midgut, which forms the rest of the small intestine as well as the cecum, ascending colon, and most of the transverse colon. The lower portion is the hindgut, which forms the descending colon, sigmoid colon, and rectum of the large intestine.
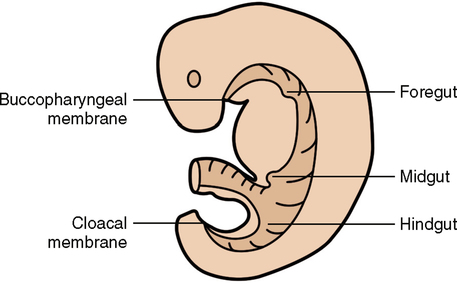
In Fig. 18-2, you can see the foregut with the tube still closed at the top and the hindgut at the bottom as well. Eventually, at about 4½ weeks, the upper end of the tube breaks down and connects with the primitive oral cavity, which is a depression known as the stomodeum, and forms the oral cavity and oral pharynx. At about 6 to 7 weeks, the bottom end of the tube breaks down and becomes the anal and urethral openings. The point in Fig. 18-2 where the foregut region and the stomodeum share a common wall is known as the buccopharyngeal membrane. This membrane is found in the location that will become the region between the palatine tonsils and an area about two thirds of the way back from the tip of the tongue. When the buccopharyngeal membrane breaks down at about 4½ weeks, the connection between the oral cavity and the digestive tract is established.
FACIAL DEVELOPMENT
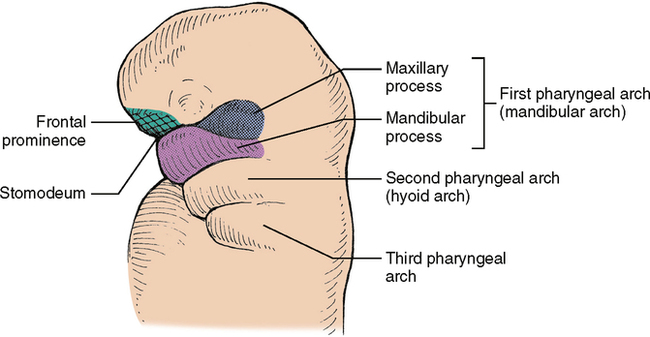
The upper two pharyngeal arches, numbered with Roman numerals I and II, are also known respectively as the mandibular and hyoid arches. First, the mandibular arch begins to show growth from the upper surface of the posterior end of the arch and will become the maxillary process. When that begins to happen, it can be subdivided into mandibular processes below and maxillary processes above (Fig. 18-3). The mandibular processes will form the mandible, and the maxillary processes will form the maxillae, the zygomatic bones of the cheek, and the palatine bones, which form the hard palate in the roof of the mouth. The maxillae also comprise the upper jaw.
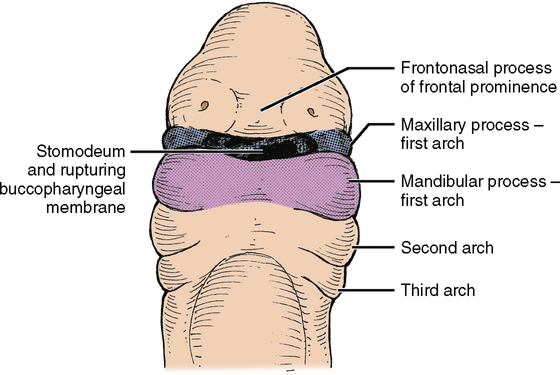
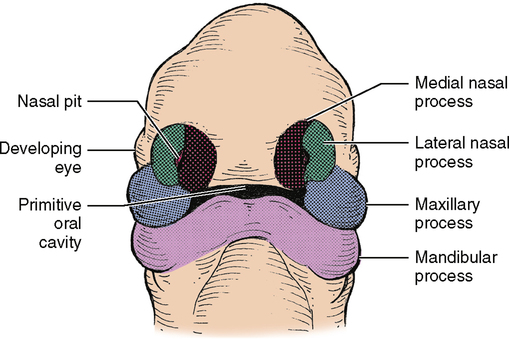
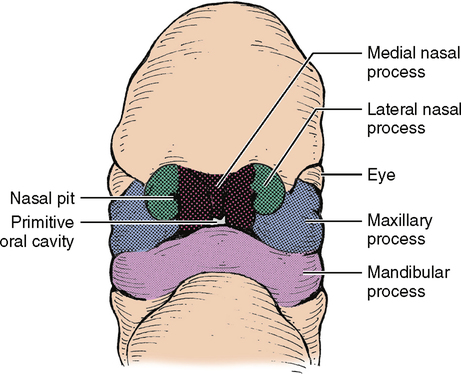
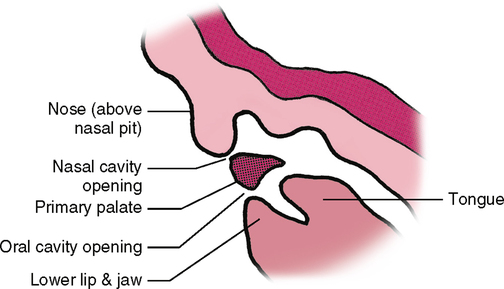
In the anterior (frontal) view of a 3-week embryo, notice the forehead area, known as the frontal prominence, the stomodeum (primitive oral cavity), and the mandibular processes of the mandibular arch (Fig. 18-4). During the fourth embryonic week, some changes can be seen. First, two small depressions form low on the frontal prominence; these are the nasal pits, the beginning of the nasal cavities. The areas on either side of these nasal pits begin to form a ridge and become the medial and lateral nasal processes (Fig. 18-5). From the side of the head, notice that the maxillary processes are starting to enlarge slightly and seem to be growing toward the midline. By the sixth week the two medial nasal processes have fused together and, along with the two maxillary processes, have formed the upper lip (Fig. 18-6). The lateral nasal process takes no part in forming the upper lip. It gets pushed up and out of the way. Also about this time the nasal pits deepen until they open into the primitive oral cavity at about 6 weeks (Fig. 18-7).
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


