18
Class III malocclusion
INTRODUCTION
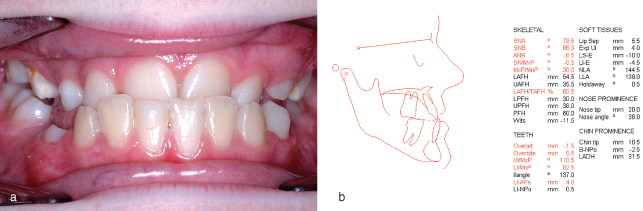
A Class III incisor relationship exists when the lower incisor edges occlude anterior to the cingulum plateau of the palatal surface of the upper incisors (Figure 18.1a; British Standards Classification). The overjet is reduced and may be reversed. The prevalence of Class III malocclusion in the UK is 3.2%.1
Figure 18.1 (a) Class III incisor relationship. (b) Lateral cephalometric analysis demonstrating Class III skeletal base relationship.
AETIOLOGY
Class III malocclusion can have a strong genetic predisposition and hence may run in families. Usually an anteroposterior Class III skeletal base relationship, due to maxillary retrusion and/or mandibular protrusion, accompanies a Class III malocclusion with a reduced or negative ANB angle (Figure 18.1b). Cases with increased Frankfort-mandibular planes angle (FMPA) and anterior open bite require more complex management than those with decreased vertical proportions, while bilateral buccal crossbites usually reflect a transverse maxillary deficiency.
The soft tissues encourage dentoalveolar compensation. The tongue proclines the maxillary incisors, while a strong lower lip retroclines the mandibular incisors to try to achieve incisor contact. Rarely, a Class III malocclusion may result from retroclined upper and lower incisors on a Class I skeletal base.2
ASSESSMENT
In addition to detailing the patient’s concerns, it is important to question both the patient and their parents about the presence of skeletal disharmonies in any relatives as the patient may also exhibit the same at the completion of growth.
A comprehensive clinical examination should include extra- and intraoral components. The anteroposterior skeletal base relationship and the vertical facial proportions should be assessed with the patient in natural head position. Profile disharmonies (Figure 18.2) and any facial/dental asymmetries should be noted. To supplement the clinical examination, a lateral cephalogram should be analysed (Figure 18.1b),3 which may support whether the case can be treated by orthodontics, or where orthognathic surgery is required.
Figure 18.2 Typical facial profile characterised by a retrusive maxilla in a severe Class III malocclusion.

Minimal or no overbite is a poor prognostic factor for orthodontic success. Conversely, a deep overbite is helpful in the retention of the corrected incisor relationship.
TREATMENT (TABLE 18.1)
Primary Dentition
There is no evidence to suggest that orthodontic intervention during the primary dentition avoids, or reduces, the complexity of later orthodontic treatment.
Table 18.1 Management of Class III malocclusion
| Clinically | Management |
| Early mixed dentition | |
| Incisor crossbites | |
| Retained primary incisors | Extract retained primary teeth |
| Premature contact and mandibular displacement | Extract or grind cusp tips (usually primary canines) |
| Procline maxillary permanent incisor(s) using an upper removable appliance (URA) or a fixed appliance | |
| Late mixed dentition | |
| Proclined lower incisors | URA incorporating inverted labial bow |
| Class III incisors with deep overbite and mild/moderate skeletal Class III | Protraction headgear and rapid maxillary expansion |
| Early permanent dentition | |
| Mild/moderate skeletal discrepancy | Procline maxillary permanent incisors using URA/fixed appliance |
| – no concern about facial appearance | Camouflage skeletal pattern using fixed appliances |
| Postpone treatment decision until skeletal growth completed | |
| Severe skeletal discrepancy or a concern about facial appearance | Accept malocclusion will require combined orthodontic treatment/orthognathic surgery in adulthood |
| Align maxillary arch with fixed appliance and relieve crowding, accepting Class III incisor relationship will require orthognathic surgery in adulthood | |
| Adult treatment | |
| Mild/moderate skeletal discrepancy | Procline maxillary permanent incisors using URA/fixed appliance |
| – no concern about facial appearance | Camouflage skeletal pattern using fixed appliances |
| Severe skeletal discrepancy or a concern about facial appearance | Combined orthodontic treatment/orthognathic surgery |
Early Mixed Dentition Treatment
Where permanent incisors erupt palatally to their predecessors, the retained primary teeth should be removed. Class III incisor relationships resulting from a premature contact and subsequent mandibular shift should also be treated early due to the association between childhood crossbites and adult temporomandibular joint dysfunction.4 Frequently, the primary canines are the prematurely contacting teeth requiring cuspal grinding or extraction. If the prematurely contacting teeth are permanent incisors, wear facets may occur. In this si/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


