Permanent Anterior Teeth
Learning Objectives
• Demonstrate the correct location of each permanent anterior tooth on a diagram and a patient.
• Use and pronounce the key terms when discussing the permanent anterior teeth.
New Key Terms
Avulsion (ah-vul-shin)
Cingulum (sin-gu-lum)
Cusp slope (kusp), tip
Cuspid (kus-pidz)
Developmental depressions, groove, pits (di-ah-ste-mah)
Diastema (di-ah-ste-mah)
Fossa (fos-ah) (plural, fossae, fos-ay)
Hutchinson’s incisors (hutch-in-suns in-sigh-zers)
Impacted (im-pak-ted)
Incisal angle (in-sign-sl), edge, ridge
Mamelons (mam-ah-lons)
Mesiodens (me-ze-oh-denz)
Peg lateral (lay-be-al), lingual, marginal
Ridge: labial (lay-be-al), lingual, marginal
Supplemental groove
Permanent Anterior Teeth
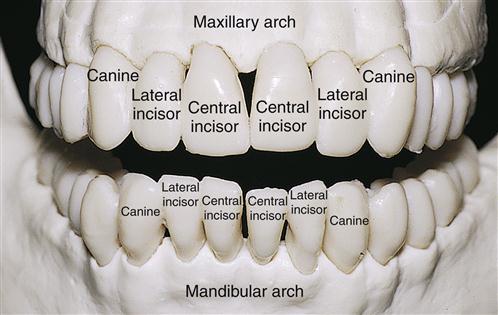
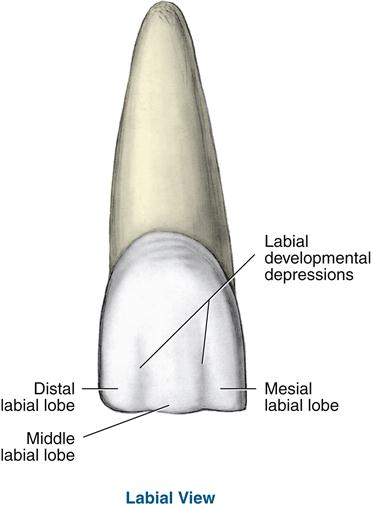
Permanent anterior teeth include the incisors and canines (Figure 16-1, see Figure 2-4, 15-1). All anterior teeth are composed of four developmental lobes: three labial lobes named mesiolabial, middle labial, and distolabial, and one lingual lobe (Figure 16-2). Two vertical labial developmental depressions outline the separations among the labial developmental lobes, the mesiolabial and distolabial developmental depressions. All permanent anterior teeth are succedaneous, which means that each one replaces the primary tooth of the same type. The development of the permanent dentition is discussed in Chapter 6.
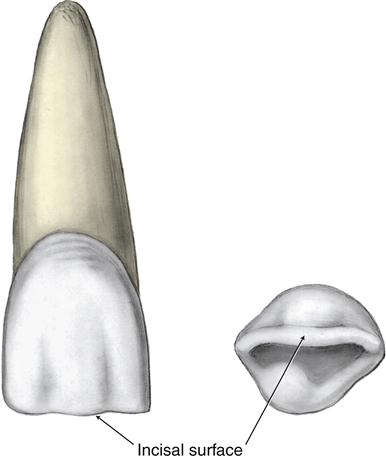
The long crown of an anterior tooth has an incisal surface, which is its masticatory surface (Figure 16-3). From the labial and lingual, the crown outline is trapezoidal, or four-sided, with only two parallel sides. The longer of the two parallel sides is toward the incisal.
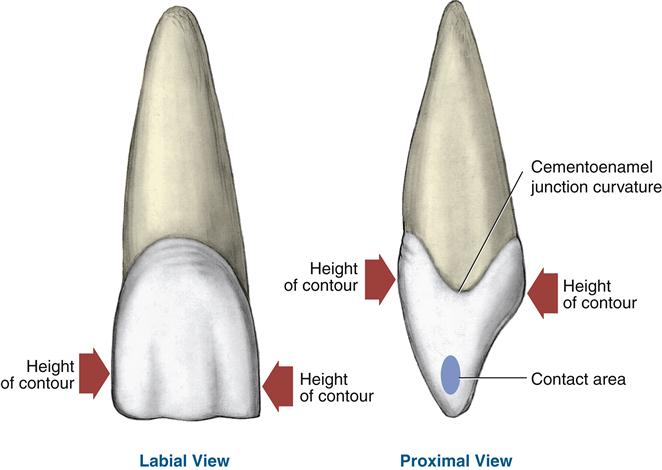
The crown outline is triangular when viewed from the proximal, with the base of the triangle at the cervical and the apex at the incisal edge (Figure 16-4). These teeth are wider mesiodistally than labiolingually when compared with posteriors. For anteriors, the height of contour, or crest of curvature, for both the crown’s labial and lingual surfaces is in the cervical third. Each contact area of anteriors is usually centered labiolingually on their proximal surfaces and has a smaller area than the contacts of posterior teeth (see Figure 15-10). On each proximal surface, the cementoenamel junction (CEJ) curvature of all anteriors is greater than that of the posteriors.
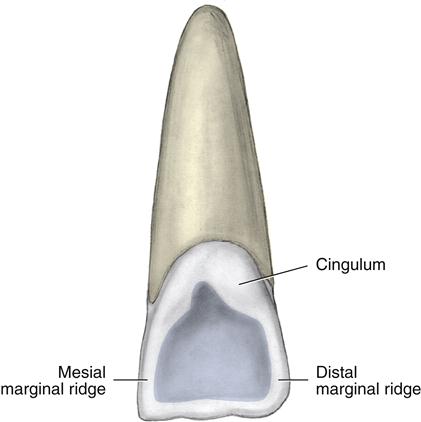
The lingual surfaces of all anteriors have a cingulum (Figure 16-5). The cingulum is a raised, rounded area on the cervical third of the lingual surface in varying degrees of prominence or development on anteriors. The cingulum corresponds to the lingual developmental lobe. Ridges may also be present on the lingual surface. The lingual surface on anteriors is bordered mesially and distally on each side by a rounded raised border, the marginal ridge.
Some anteriors have a more complex lingual surface with a fossa or even fossae, which are shallow, wide depressions (Figure 16-6). Some may also have developmental pits, which are located in the deepest part of each fossa. Other anteriors may have on their lingual surface a developmental groove, or primary groove, a sharp, deep, V-shaped linear depression that marks the junction among the developmental lobes.
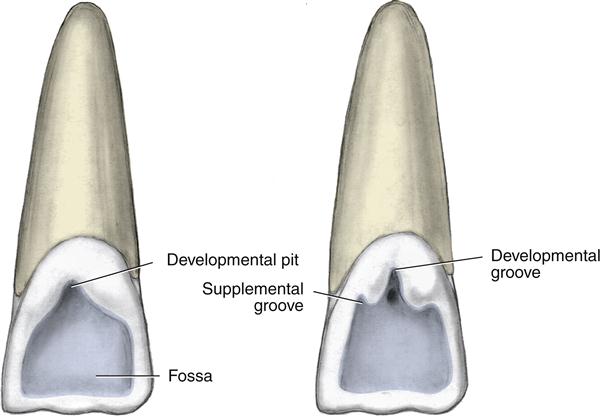
In addition, a supplemental groove, or secondary groove, may also be present on the lingual surface of anteriors (Figure 16-6).
 Clinical Considerations for Anterior Teeth
Clinical Considerations for Anterior Teeth
Patients may have difficulty in maintaining homecare of anteriors because their dental arch position naturally may allow the lips to overhang the teeth. Thus, patients may clean only the incisal two-thirds of the crowns of anteriors with their toothbrushes, missing the associated cervical area and facial gingival tissue. This overhanging of the lips may also make instrumentation difficult.
Instrumentation may also be compromised in the area where the greater curvature of the CEJ is present interproximally on anteriors, where accessibility is limited and the teeth are in close proximity. The grooves on the lingual surface of anteriors may present areas for dental biofilm retention if they extend to the root and are near the adjacent gingival tissue; for this reason, the grooves may be reduced with a dental bur during a minor odontoplasty.
When the anterior teeth are restored, the Golden Proportions can be useful guidelines to balance the size of the teeth with one another. These guidelines designate that the ideal width of the maxillary lateral incisor as a factor of 1.0×, the width of the central incisors as 1.618×, and the width of the canines as 0.168× when observed in two dimensions from the facial aspect. Other formulas state that the maxillary central should be 60% wider than the lateral, and the lateral should be 60% wider than the canine from its midline to its mesial aspect. In addition, each incisor should also ideally have an 8:10 width-to-length ratio.
In addition, consideration of smile design may involve the drawing of a line following the ideal outline formed by the incisal edges of the maxillary anterior teeth; this line should be 1 to 3 mm parallel or equidistant to the lower lip line. Some variation will occur with aging. Older patients lose elasticity in the lips, which results in sagging, prominence of the mandibular teeth, and diminution of the maxillary teeth. Straight smiles are perceived as more masculine and feminine smiles as more curved. In addition, if the upper lip line appears to be convex instead of concave compared with the lower lip line, the smile will be perceived as more youthful (see Figure 14-22).
This is a shallower, more irregular linear depression. Supplemental grooves branch from the developmental grooves but are not always present in the same pattern on each different tooth type. In general, the more anterior the tooth is located in the arch, the fewer supplemental grooves are present and the smoother the lingual surface.
Anteriors usually have a single root, with some exceptions. Each root of the maxillary anterior teeth has great lingual and slight distal inclination (see Figure 20-9). Each root of the mandibular anterior teeth varies in angulation from nearly vertical to great lingual inclination, with the canines possibly having a slight distal root inclination.
Permanent Incisors
General Features
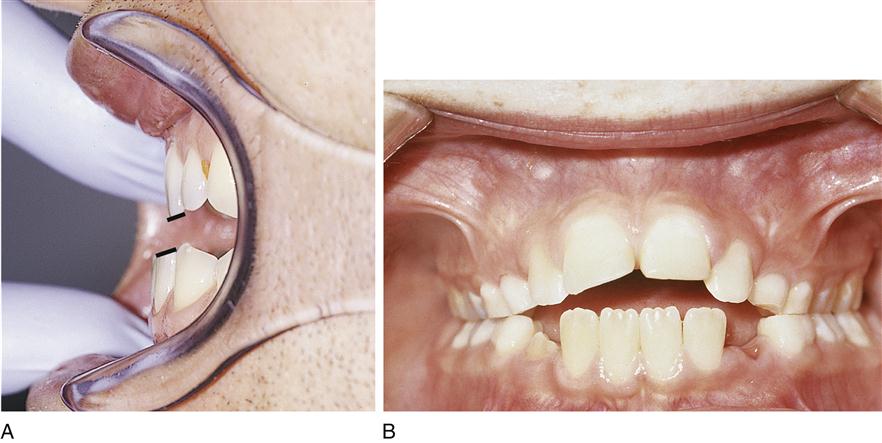
Permanent incisors are the eight most anterior teeth of the permanent dentition, with four in each dental arch (Table 16-1). The two types are the central incisors and the lateral incisors. The centrals are closest to the midline, and the laterals are the second teeth from the midline. One of each type is present in each quadrant of each dental arch. Both types are mesial to the permanent canines when the permanent dentition is fully erupted. The permanent incisors are succedaneous and replace the primary incisors of the same type. On occasion, the permanent incisors seem to spread out across the arch as a result of spacing during initial eruption and with the eruption of the permanent canines, these spaces often close. When newly erupted, each incisor also has three mamelons, or rounded enamel extensions on the incisal ridge from the labial or lingual views (Figures 16-7 and 16-8, B). The mamelons are extensions from the three labial developmental lobes.
TABLE 16-1
Anatomical Information on Permanent Incisors
| MAXILLARY CENTRAL INCISOR | MAXILLARY LATERAL INCISOR | MANDIBULAR CENTRAL INCISOR | MANDIBULAR LATERAL INCISOR | |
| Universal number | #8 and #9 | # 7 and #10 | # 24 and #25 | #23 and #26 |
| General crown features | Incisal edge and incisal angles | |||
| Specific crown features | Widest crown MD, greatest CEJ curve, and height of contour; distal offset cingulum, shallow lingual fossa, marginal ridges | Greatest crown variation, like a smaller maxillary central, prominent lingual surface; centered cingulum, pronounced marginal ridges | Smallest and simplest tooth, bilaterally symmetrical; small centered cingulum, subtle lingual fossa, and equal subtle marginal ridges | Like a larger mandibular central, not bilaterally symmetrical; appears twisted distally; small, distally placed cingulum; lingual fossa and moderate mesial marginal ridge longer than distal |
| Height of contour | Cervical third | |||
| Mesial contact | Incisal third | |||
| Distal contact | Junction of incisal and middle thirds | Middle third or junction with incisal third | Incisal third | Incisal third |
| Distinguishing right from left | Sharper MI angle, rounder DI angle, more pronounced mesial CEJ curvature | |||
| General root features | Single-rooted | |||
| Specific root features | Overall conical shape; no proximal root concavities | Bow shaped on cross section; root is longer than the crown; proximal root concavities give double-rooted appearance | ||
| Rounded apex; triangular in cross section | Root curves distally, with sharp apex; oval in cross section; same or longer than central but thinner | |||
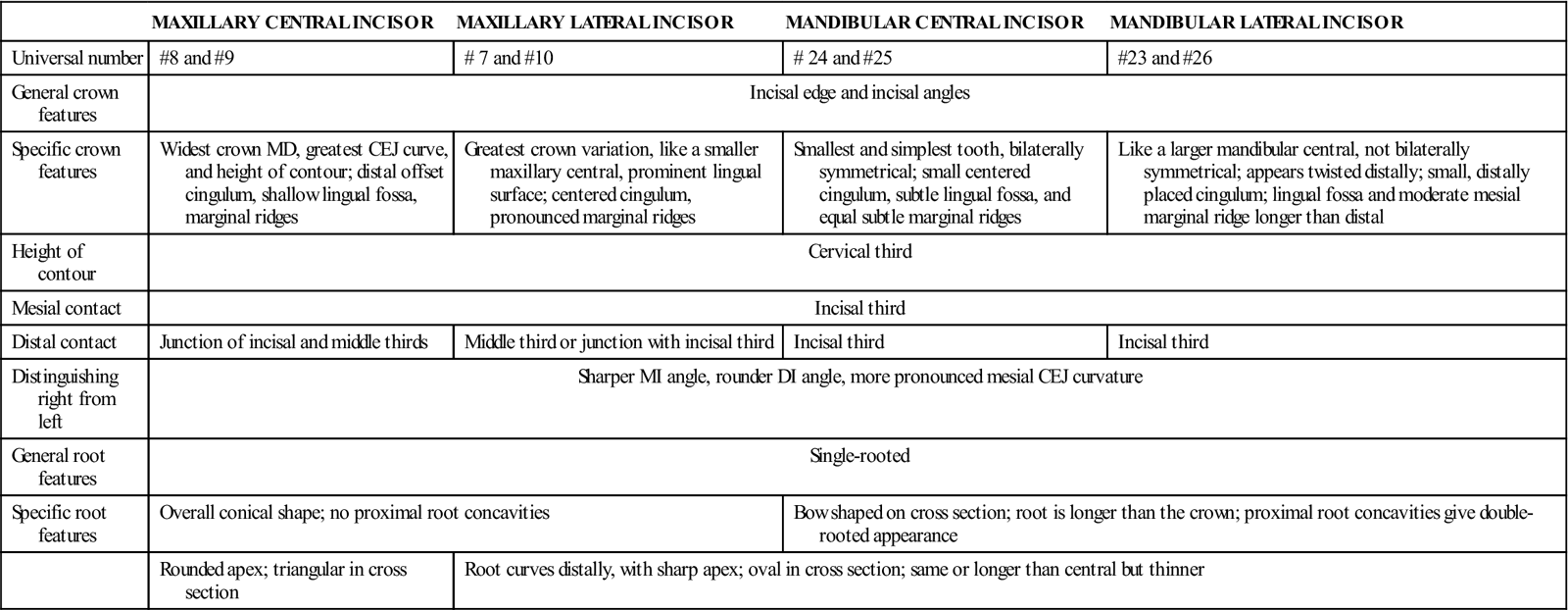
CEJ, Cementoenamel junction; DI, distoincisal; MD, mesiodistally; MI, mesioincisal.

The incisors are also the only permanent teeth with two incisal angles formed from the incisal ridge or incisal edge (discussed later) and each proximal surface. Incisors of both types are the only permanent teeth with a nearly straight incisal ridge, which is a linear elevation on the masticatory or incisal surface when newly erupted—thus the name incisors.
The lingual surface has a cingulum that corresponds to the lingual developmental lobe, although its prominence or development differs for each type of incisor. These teeth also have a lingual fossa and marginal ridges on the lingual surface, again in differing developmental levels for each type of incisor. The height of contour for both labial and lingual surfaces of all incisors is at the cervical third, as is the case for all anteriors.
Permanent Maxillary Incisors
General Features
Permanent maxillary incisors are the four most anteriorly placed teeth of the maxillary arch. Each has a crown that is larger in all dimensions, especially mesiodistally, compared with a mandibular incisor. In addition, the labial surfaces are rounder from the incisal aspect, with the tooth tapering toward the lingual.
 Clinical Considerations for Incisors
Clinical Considerations for Incisors
Incisors function as instruments for biting and cutting food during mastication, because of their incisal ridge, triangular proximal form, and arch position. They also support the lips and face, as well as maintain vertical dimension of the face. Additionally, they contribute to overall normal arch appearance. Finally, they are involved during the articulation of speech and assist in guiding jaw closure as the teeth come together.
Because of the anterior position of the incisors, esthetic concerns are important during restorative procedures. However, restorative replacement of only a part of the incisal edge of this tooth after traumatic fracture may also be difficult to maintain owing to this tooth’s function in biting and cutting food.
The mamelons on the incisal ridge of incisors usually undergo attrition, the wearing away of a tooth surface caused by tooth-to-tooth contact, shortly after eruption as the tooth moves into occlusion (Figures 16-8, A and 16-9, C, see Figure 16-17 and Chapter 20). The incisal ridge, thus, now appears flattened from its labial, lingual, or incisal views and becomes the incisal edge. Thus, mamelons are usually most noticeable immediately after eruption, becoming undetectable as the tooth undergoes attrition over time. With attrition, the maxillary incisors’ incisal edges show lingual inclination and the mandibular incisors have a labial inclination to their incisal edges. Thus, with this arrangement, the incisal edges of the maxillary and mandibular incisors are now usually parallel to one another and mesh correctly during mastication. Excessive attrition can sometimes create a bow-shaped wear pattern on the incisal edge when viewed from the incisal.

If mamelons are still present on the incisal ridge in an adult, it is because these teeth are not in occlusion, whereby they undergo normal attrition, such as with an anterior open bite relationship (Figure 16-8, B, see Figure 20-22). Thus mamelons occasionally do not wear down, especially when malalignment of the teeth and loss of tooth-to-tooth contact with occlusion exist. Many young adults do not like the appearance of mamelons and sometimes request to have them polished off; some patients even request placement of restorative materials to achieve a straight-appearing incisal edge. Part of the reason that the mamelons are so noticeable, if present long after eruption, is that these extensions are made of enamel, with no dentin layer underneath.
This factor and their thinness contribute overall to their translucent appearance, as opposed to the rest of the clinical crown, which is usually more opaque than the mamelons. Given this translucent quality, mamelons often appear to be a different shade than the rest of the tooth, sometimes making them much more distinct. With the addition of tooth whitening (bleaching), this incisal translucency may become even more noticeable.
All lingual surface features, including the marginal ridges, lingual fossa, and cingulum, are more prominent on the maxillary incisors than on the mandibular incisors. Finally, the incisal edge is just labial to the long axis of the root from either proximal view.
Each root is short compared with those of other maxillary teeth and usually is without root concavities. Bulbous and pronounced crowns may also create deep mesial and distal concavities at the CEJ.
The central and lateral incisors of the maxillary arch resemble each other more than they resemble the similar type of incisors of the opposing arch. Generally, a maxillary central incisor is larger than a maxillary lateral incisor, but overall they have a similar form. Both types of maxillary incisors are wider mesiodistally than labiolingually.
 Developmental Disturbances of Incisors
Developmental Disturbances of Incisors
The crown of a permanent incisor can be affected with dens in dente (see Table 6-3, D). This disturbance leaves the tooth with a deep lingual pit resulting from invagination of the enamel organ into the dental papilla. This pit may lead to pulpal exposure and pathology. Dens in dente may be hereditary and is more common with a maxillary lateral incisor.
The crowns of permanent incisors, similar to molars, can be affected in children with congenital syphilis. A pregnant woman infected with syphilis transmits the spirochete Treponema pallidum, a sexually transmitted microorganism, to her fetus via the placenta. This microorganism may cause localized enamel hypoplasia, which can result in Hutchinson’s incisors, occurring during tooth development (see Figure 3-16).
A Hutchinson’s incisor has a crown with a screwdriver shape from the labial view and is wider cervically and narrow incisally, with a notched incisal edge. Children may also have other developmental anomalies, such as blindness, deafness, and paralysis from congenital syphilis. Treatment of these teeth with restorative materials may improve their appearance.
A sharp, small, extra cusp, or talon cusp (claw), occasionally appears as a projection from the cingulum of incisor teeth and can happen in both dentitions. These types of cusps can interfere with occlusion; however, grinding them down is a hazardous endeavor. They often contain a prominent pulp horn, which is at an increased risk of exposure during restorative procedures.
 Clinical Considerations for Maxillary Incisors
Clinical Considerations for Maxillary Incisors
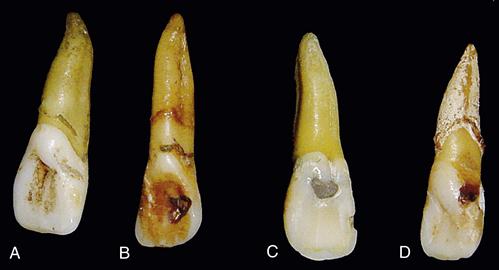
If a maxillary incisor has increased prominence of the lingual marginal ridges and a deeper lingual fossa, it may be considered a shovel-shaped incisor (Figure 16-9, A). It can also have an accentuated cingulum (Figure 16-9, B), with deepened grooves, and show incisal edge attrition (Figure 16-9, C).
Another lingual feature, if present on the maxillary incisors, a lingual pit, is at increased risk of caries development due to both increased dental biofilm retention and the weakness of the enamel forming the walls of the pit (Figure 16-10, A to C, see Chapter 12). If the lingual pit is deep, a developmental disturbance of dens in dente must be considered, and needed changes made in the patient’s treatment plan (discussed earlier). Also present may be a vertically placed linguogingival groove (Figure 16-10, D), which originates in the lingual pit and extends cervically and slightly distally onto the cingulum, and is also more common on maxillary laterals, possibly resulting in caries.
Clinicians need to be aware of these lingual pit and groove patterns on maxillary incisors when they examine a dentition in order to determine the patient’s caries risk level. All pits and grooves must be checked for decay with an explorer and mirror. Light-induced devices that measure measures changes in laser fluorescence of hard tissue allow dental professionals to better diagnose early lesions in pits and grooves. Maxillary incisors with deep pit and groove patterns but without incipient decay should have enamel sealants placed as soon as they erupt.
In addition, supragingival tooth deposits such as dental biofilm and stain can collect in the prominent lingual surface concavities of maxillary incisors (see Figure 16-9, D). During instrumentation, the proximal surfaces of these teeth are more accessible from the lingual than the facial approach because of the increased tapering of the tooth to the lingual. Dental professionals must be careful to check for deposits in any mesial and distal root concavities at the CEJ if this area is exposed as a result of recession.
Finally, many dental professionals believe that competency of the lips to maintain a lip seal, when at a resting posture, can affect the position of the maxillary incisors (see Chapter 20). Competent lips allow these tooth tips to lie below the lower lip border, helping to maintain normal inclination. Incompetent lips that fail to provide a lip seal do not control this inclination and may even allow the maxillary incisors to lie in front of the lower lip, exaggerating already buccally-inclined teeth and possibly become lingually inclined. A tongue thrust is a complicating factor that may be associated with this problem (see Chapter 20).
Permanent Maxillary Central Incisors #8 and #9
Specific Overall Features (Figure 16-11)
Permanent maxillary central incisors erupt between 7 to 8 years of age (root completion at age 10). Thus, these teeth usually erupt after the mandibular central incisors. Many child patients want these two teeth to come in fast to fill their wide arch space when they shed their four primary maxillary incisors, as in the old song, All I Want for Christmas Is My Two Front Teeth.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


