15
Recall Procedures
In this chapter, we stress the importance of planning a programme of recall appointments after fitting complete dentures, to ensure that the tissues are not being damaged and that the dentures are functioning efficiently and comfortably. A recall visit also gives the patient an opportunity to seek advice over any concerns.
Short-term and long-term recalls are considered separately.
Short-term recall
The first recall appointment should be no longer than 1 week after fitting the dentures. At this visit it is necessary to obtain a careful history of any complaint, such as pain or looseness of the dentures, and to undertake a thorough examination.
The patient’s complaints
The clinician should routinely enquire about the patient’s progress during the first week of denture wearing. This is important because the more timid patient may need positive encouragement before being willing to comment about a matter of concern. Of course, there are other patients who require no such invitation and will have already composed a list of difficulties. However, even then the routine enquiry about progress is likely to be welcomed as an example of a caring ‘after-sales service’.
Whatever the type of patient response, advice and explanation by the clinician may be all that are needed to overcome certain denture problems, particularly if the patient is an inexperienced denture wearer. Other problems will require intervention to modify the dentures.
Problems with the dentures may be caused by faults that passed unnoticed at the fit stage, or by changes occurring in the mouth since that time. There can also be persistent difficulties caused by insurmountable hurdles related to unfavourable anatomy, unrealistically high patient expectations, or lack of adequate denture control skills.
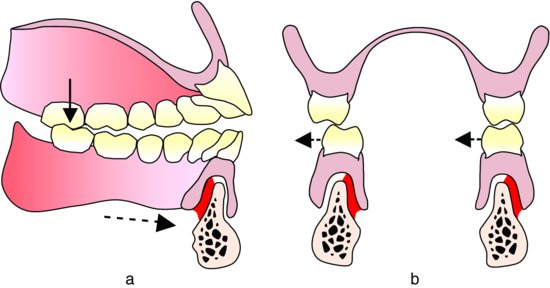
Figure 15.1 (a) A posterior premature contact, resulting in forward movement of the lower denture (dotted arrow), produces inflammation of the mucosa on the lingual aspect of the alveolar ridge in the anterior region. (b) Lateral displacement of the lower denture produces inflammation of the mucosa in areas closely related to the occlusal error.
The more common complaints are:
- Discomfort
- Looseness
- Appearance
- Speech
The first two problems occur most frequently. The last two are dealt with elsewhere in the book.
Discomfort
Examples of injury to the mucosa which arise from faults on the impression surface include mucosal damage in the sulcus due to over-extension, and on the most bulbous part of a ridge where the denture base has been inadequately relieved from a bony undercut. Where there is a clear relationship between mucosal damage and the impression surface, appropriate correction of the denture should be undertaken. It may be tempting to assume that all mucosal damage is directly related to faults in the impression surface. However, such an assumption would be fraught with danger as the damage could be equally due to faults in the occlusion causing movement of the denture or concentrations of occlusal pressure. It is important to appreciate that the occlusal error causing a problem may be some distance from the site of inflammation (Fig. 15.1). It is also important to remember that when there is a complaint of discomfort an assessment of the occlusion must always be made before any adjustment of the impression surface is carried out.
Looseness
Looseness of the dentures may occur because the patient has not, as yet, learned to control the new shapes in the mouth, rather than being due to denture faults or anatomical shortcomings. Thus, a check must be made on the patient’s progress in adapting to the new dentures. Bearing in mind that 20% of experienced denture wearers require up to a month in which to become proficient with their new dentures (Bergman & Carlsson 1972), it is likely that a significant number of patients will benefit from the offer of further advice, reassurance and follow-up.
Routine checks and treatment
Checks that should always be made at the recall appointment when carrying out an examination of the patient’s mouth and dentures are:
- Occlusion
- Tissue health
- Denture cleanliness
Occlusion
It must be remembered that because new dentures are seated on a surface which is compressible and liable to change, the initial few days of function may have caused an alteration in the occlusion. Such an alteration is a potent cause of mucosal injury, and it can also lead to problems with the masticatory muscles. Patients attempt to adapt to an uneven occlusion by altering the normal pattern of mandibular movement. Such an attempt is liable to produce muscular disorders which, in the short term, may pass unnoticed by the patient, but in the longer term can give rise to significant discomfort. Methods of carrying out occlusal adjustment are described in Chapter 14.
Tissue health
Even if the patient expresses complete satisfaction and reports perfect comfort, it is essential to carry out a thorough examination to check on tissue health. This is because occasionally there may be mucosal injury, even frank ulceration, without the patient apparently being aware of it. The absence of a complaint under such circumstances may be due to a high pain threshold or a desire to please. With the information gleaned from the history and an examination, a diagnosis of any problem should be established and appropriate treatment decided upon.
The impression surface of the denture should never be adjusted in an empirical manner. Once any occlusal faults have been eliminated, a further check of the impression surface should be made using a pressure-disclosing medium. If this sequence is not carried out, it is difficult to judge whether an area of inflammation is due either to an impression surface defect or to an occlusal error. Pressure-disclosing media suitable for this purpose include silicone rubber materials formulated for the purpose, pressure-disclosing paste or wax and low viscosity alginate.
If the mucosal damage has been diagnosed as being due to a fault with the impression surface and is localised, a disclosing material is applied to the impression surface of the denture in the suspect area. The denture is then seated firmly for a few seconds and on removal any pressure points are indicated by the pink denture base showing through the material. Adjustment of the impression surface can then be carried out in a relatively precise manner.
If the mucosal damage is more generalised, an alternative technique which is simple, quick and revealing is to obtain a wash impression over the whole of the impression surface using a low viscosity mix of alginate or silicone rubber. The set impression gives a clear picture of pressure points and base extension. Any pressure points can be marked with a pencil before the material is removed allowing their precise correction. If adhesive has not been applied to the denture beforehand, the impression can then be quickly and cleanly removed from the denture after the adjustments have been completed.
Denture cleanliness
A check on denture plaque control can be made by direct visual inspection assisted where necessary by the use of a disclosing solution. If there are significant deposits it is essential to discover what cleaning technique the patient is using. Reinforcement of advice at this stage may prevent the development of denture-induced stomatitis, angular stomatitis, staining of the dentures and mouth odour. If there have been significant problems at the first recall appointment, a further appointment for short-term review should be made to check on progress. The clinician can also ensure that a/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


