The First Stage of Comprehensive Treatment
Alignment and Leveling
GOALS OF THE FIRST STAGE OF TREATMENT
Principles in the Choice of Alignment Arches
Properties of Alignment Archwires
Alignment of Symmetric Crowding
Individual Teeth Displaced Into Anterior Crossbite
Transverse Maxillary Expansion by Opening the Midpalatal Suture
The idea of dividing comprehensive orthodontic treatment into stages, which makes it easier to discuss technique, was emphasized by Raymond Begg.1 The three major stages he proposed are used to organize this section because they still apply reasonably well to treatment with the modern edgewise appliance that now is used almost universally. These stages are: (1) alignment and leveling, (2) correction of molar relationship and space closure, and (3) finishing. The latter two stages are covered in Chapters 15 and 16, respectively. Not every patient will require the steps of each treatment stage, but whatever the technique, it is likely that both the archwires and the way they are utilized will be changed at the various stages. Even with the most cleverly preadjusted edgewise appliance, a change of archwires will be needed before the finishing stage is reached, and some archwire adjustments are quite likely to be necessary in finishing.
Goals of the First Stage of Treatment
Treatment for any patient should be undertaken only after a thorough analysis of the patient’s problems, the preparation of a treatment plan to maximize benefit for that patient, and the development of a sequence of orthodontic treatment steps (archwires and their activation [i.e., mechanotherapy]) to produce the desired result. The diagnostic and treatment planning procedure outlined in Chapters 6 and 7, which culminates in an outline of the steps in treatment, is recommended.
In almost all patients with malocclusion, at least some teeth are initially malaligned. The great majority also have either excessive overbite, resulting from some combination of an excessive curve of Spee in the lower arch and an absent or reverse curve of Spee in the upper arch, or (less frequently) anterior open bite with excessive curve of Spee in the upper arch and little or none in the lower arch. The goals of the first phase of treatment are to bring the teeth into alignment and correct vertical discrepancies by leveling out the arches. In this form, however, neither goal is stated clearly enough. For proper alignment, it is necessary not only to bring malposed teeth into the arch but also to specify and control the anteroposterior position of incisors, the width of the arches posteriorly, and the form of the dental arches. Similarly, in leveling the arch, it is necessary to determine and control whether the leveling occurs by elongation of posterior teeth, intrusion of incisors, or some specific combination of the two. The form of the dental arches obviously varies between individuals. Although the orthodontist has some latitude in changing arch form and indeed must do so in at least one arch if the upper and lower arch are not compatible initially, more stable results are achieved when the patient’s original arch form is preserved during orthodontic treatment (see Chapter 9 for a discussion of arch form and archwire shape). The light resilient archwires used in the first stage of treatment need not be shaped to the patient’s arch form as carefully as the heavier archwires used later in treatment, but from the beginning, the archwires should reflect each individual’s arch form. If preformed archwires are used for alignment (as is usually the case because superelastic nickel–titanium [A-NiTi] wires must be preformed), the appropriate large, medium, or small arch form should be selected.
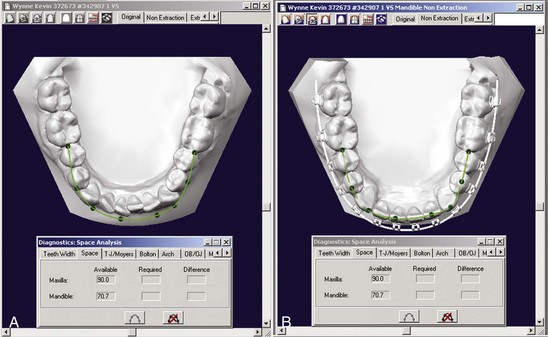
Because the orthodontic mechanotherapy will be different, depending on exactly how alignment and leveling are to be accomplished, it is extremely important to clearly visualize the desired position of the teeth at the end of each stage of treatment before beginning that stage. Computer programs now exist to make this easier (Figure 14-1), but it is the thought process that counts. For instance, the best alignment procedures will result in incisors that are far too protrusive if the extractions necessary to prevent protrusion were not part of the plan. Similarly, unless leveling by intrusion is planned when it is needed, the appropriate mechanics are not likely to be selected.
Alignment
Principles in the Choice of Alignment Arches
1. Initial archwires for alignment should provide light, continuous force of approximately 50 gm to produce the most efficient tipping tooth movement. Heavy force, in contrast, is to be avoided.
2. The archwires should be able to move freely within the brackets. For mesiodistal sliding along an archwire, at least 2 mil clearance between the archwire and the bracket is needed, 4 mil clearance is desirable, and more than that provides no advantage. This means that the largest initial archwire that should be used with an 18-slot edgewise bracket is 16 mil, and 14 mil would be more satisfactory. With the 22-slot bracket, a 16 or 18 mil archwire would be satisfactory if they delivered the correct force. Whatever the archwire, it should be held loosely in the bracket; however, as we have pointed out in Chapter 9, friction is not the major component of resistance to sliding, and the claim that more rapid alignment is a major advantage of self-ligating brackets has been shown to be incorrect.
3. Rectangular archwires, particularly those with a tight fit within the bracket slot so that the position of the root apex could be affected, normally should be avoided. The principle is that it is better to tip crowns to position during initial alignment rather than displacing the root apices; the corollary is that although a highly resilient rectangular archwire, such as 17 × 25 superelastic NiTi (A-NiTi), could be used in the alignment stage, this is not advantageous because the rectangular archwire can create unnecessary and undesirable root movement during alignment (Figure 14-2). Superelastic NiTi wires have such low torsional strength that for all practical purposes they cannot torque roots,2 so this complication is uncommon, but mesiodistal movement of the root apices can and does occur, and this tends to slow the tipping movements needed for alignment. Round wires for alignment are preferred (Figure 14-3). There is no reason to pay extra for a high-performance rectangular wire for initial alignment, when alignment with it predictably will be slower and possibly more damaging to the roots than with a smaller round wire.
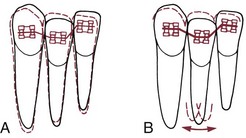
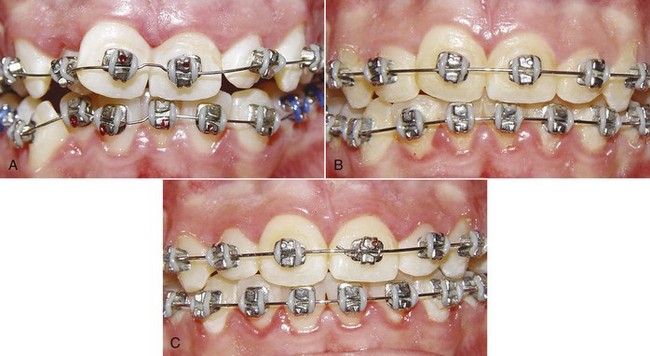
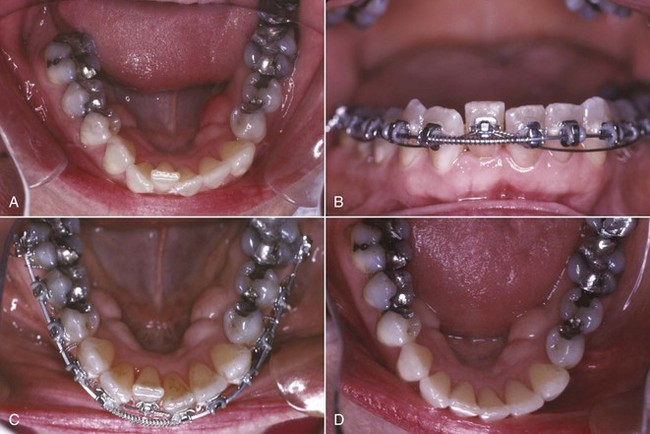
FIGURE 14-3 The sequence of alignment with a fixed appliance, in this case using Tip-Edge brackets (see Chapter 10). A, The initial superelastic round wire (16 mil A-NiTi), which was preformed with a midline bend to prevent archwire travel. B, 16 steel for final alignment 2 months later. C, Alignment completed 3 months later.
4. The springier the alignment archwire, the more important it is for the crowding to be at least reasonably symmetric. Otherwise, there is a danger that arch form will be lost as asymmetrically irregular teeth are brought into alignment. If only one tooth is crowded out of line or if an impacted tooth has to be brought into alignment—a more severe version of the same thing—a rigid wire is needed so that arch form is maintained except where springiness is required, and an auxiliary wire should be used to reach the malaligned tooth. This important point is discussed in some detail below.
Properties of Alignment Archwires
The wires for initial alignment require a combination of excellent strength, excellent springiness, and a long range of action. Ideally, there would be an almost flat load-deflection curve, with the wire delivering about 50 gm (the optimum force for tipping) at almost any degree of deflection. The variables in selecting appropriate archwires for alignment are the archwire material, its size (diameter or cross-section), and the distance between attachments (interbracket span; see Chapter 9).
At this point, superelastic A-NiTi wires are so much more effective and efficient than any alternative that there is no reason to discuss any other archwire material for alignment. The key to their success is their ability to deliver light force over a long range. The use of multiple strands of steel wire was a way to improve the performance of steel wires in initial alignment; now multiple strands of A-NiTi are being used to deliver lighter force with an archwire that is stronger and has better resistance to fracture (see Figure 14-3). Since the manufacturer’s preparation of the material determines the clinical performance, wire size is a concern primarily with respect to clearance in the bracket slot and fracture resistance. Although a 16 mil A-NiTi wire can be stiffer and deliver more force than a differently prepared 18 mil wire, that would not be possible across the total range of wire sizes, so wire size is a consideration, just less important in selecting an A-NiTi wire.
As we have discussed in Chapter 9, it is logical to use narrow (single) brackets with 18-slot edgewise and wider (twin) brackets with 22-slot. Prior to almost routine use of superelastic wires, bracket slot size and interbracket span were such strong influences on archwire choice that different initial wires often were used with the 18- and 22-slot appliances. This is no longer the case. But with superelastic wires, it is necessary to pay more attention to maintaining arch form during alignment to the point that alignment when crowding is reasonably symmetric now must be viewed differently from alignment in highly asymmetric situations.
Alignment of Symmetric Crowding
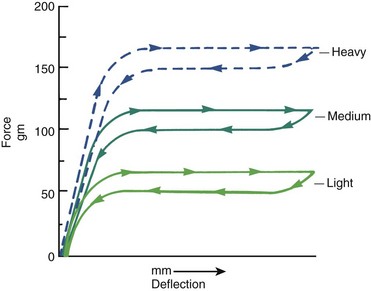
The flat load-deflection curve of superelastic NiTi (Figure 14-4) makes it ideal for initial alignment when the degree of crowding is similar on the two sides of the arch. The superelastic wire provides remarkable range over which a tooth can be moved without generating excessive force. Under most circumstances, initial alignment can be accomplished simply by tying 14 or 16 mil A-NiTi that delivers about 50 gm into the brackets of all the teeth (see Figure 14-3). It must be kept in mind, however, that alignment requires opening space for teeth that are crowded out of the arch. There are two ways to do this: use a crimped stop on the wire just in front of the molar tube so that the archwire is “proud” (slightly advanced from the crowded incisors) or use coil springs to open space (Figure 14-5). If this is done, the springs must deliver only light force to prevent distortion of arch form. The size of the superelastic wire is not a critical variable if it delivers the desired ≈50 gm force, except that 18 mil wires should not be used in the 18-slot appliance.


The reason for this surprisingly good clinical performance by the multistrand steel wire probably is that flexible archwires allow the teeth to move relative to each other during chewing, as alveolar bone bends under masticatory loads (see Chapter 8). This releases binding and allows the bracket to slide along the archwire to the next point at which binding occurs. But the lower cost of the steel archwire is quickly overbalanced by the additional clinical time necessary to retie it, especially if it must be taken out, adjusted to remove any areas of permanent distortion, and then re-ligated.
As one might expect, the extreme springiness of superelastic wires is not a totally unmixed blessing. When these wires are tied into a malaligned dental arch, they have a tendency to “travel” around the arch as the patient chews, especially if function is mostly on one side. Then the wire sticks out the back of the molar tube on one side and may come out of the tube on the other side. Occasionally, this can be extreme enough to produce the kind of situation Mark Twain called “marvelous and dismaying” (Figure 14-6, A). Archwire travel can be prevented by crimping a stop tightly onto the archwire between any two brackets that are reasonably close together (Figure 14-6, B) or by cinching the end of the wire with a special plier that will bend the NiTi wire. A stop of this type should be used routinely on initial superelastic wires.


Alignment in Premolar Extraction Situations
In patients with severe crowding of anterior teeth, it is necessary to retract the canines into premolar extraction sites to gain enough space to align the incisors. In extremely severe crowding, it is better to retract the canines independently before placing attachments on the incisors. If maximum anchorage is needed, this can be done most efficiently now with skeletal anchorage from bone screws in the alveolus (Figure 14-7).


In less extreme but still severe crowding, it is possible to simultaneously tip the canines distally and align the incisors. This can be obtained with an A-NiTi archwire coupled with A-NiTi coil springs from the first molars to tip the canines distally (Figure 14-8). The archwire must be one that was preformed by the manufacturer to have an exaggerated reverse curve of Spee, in order to limit forward tipping of the molars. This provides a way to pit distal tipping of the canines against forward bodily movement of the molars, although the moment across the molar tube will not be enough to totally prevent mesial tipping.

Alignment in Nonextraction Situations
The most straightforward way to accomplish this is to crimp a stop on the wire at the molar tube, so that it holds the wire just in front of the incisors (see Figure 14-3). At subsequent appointments, if more arch length is needed, an additional stop or stops can be quickly slipped into position, without removing the wire. When a broad arch form is used, transverse expansion across the premolars will occur. Even so, this type of arch expansion has the potential to carry the incisors facially, and so it is not indicated in the presence of severe crowding unless incisor protrusion is desired.
An alternative is to bypass the brackets on teeth that are crowded lingually, and place coil springs over the A-NiTi archwire to generate space (see Figure 14-3, D). When this is done, the archwire must be free to slide forward through the molar tubes and must be slightly long initially so that it will not come completely out of the tubes. The coil spring force must be very light to prevent distortion of arch form, but it is a misconception that the force is so light the incisors will not be proclined. They will be, just as they are when advanced stops are used. Importantly, this technique must be modified as described below if the crowding is significantly asymmetric.
Asymmetric Crowding
It is easy to add a small diameter superelastic wire as an auxiliary spring, so that a stiff main arch (16 or 18 steel) can be tied into all the teeth except the displaced one (or two—the same system works with small segments of two teeth). A segment of superelastic NiTi can be laid in the brackets on top of the main archwire, or tied below the brackets of the anchor teeth, and tied to the bracket on the displaced tooth (Figure 14-9). Some modern brackets even provide an accessory horizontal tube for this purpose (see Figure 10-35). With this arrangement, the correct light force to bring the displaced tooth into alignment is provided by the NiTi wire, and the reciprocal force is distributed over all the rest of the teeth. The result is efficient movement of the displaced tooth, with excellent preservation of arch form. When the displaced tooth is nearly into proper position, the steel base arch can be discarded and the NiTi auxiliary tied into the bracket slots.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


