Contemporary Orthodontic Appliances
Removable Appliances
The Development of Removable Appliances
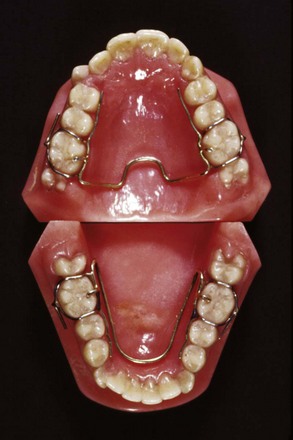
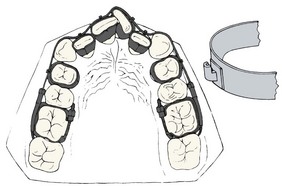
In the United States, the original removable appliances were rather clumsy combinations of vulcanite bases and precious metal or nickel-silver wires. In the early 1900s, George Crozat developed a removable appliance fabricated entirely of precious metal that consisted of an effective clasp for first molar teeth, heavy gold wires as a framework, and lighter gold fingersprings to produce the desired tooth movement (Figure 10-1). The Crozat appliance attracted a small but devoted following, and as the twenty-first century began, a modified version still was being used for comprehensive treatment by a few practitioners. Its limitation is that, like almost all removables, it produces mostly tipping of teeth. It had little impact on the mainstream of American orthodontic thought and practice, however, which from the beginning was focused on fixed appliances.
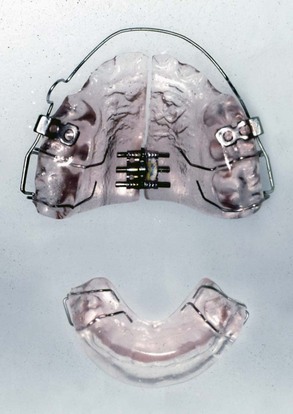
A major part of European removable appliance orthodontics of this period was functional appliances for guidance of growth. A functional appliance by definition is one that changes the posture of the mandible, holding it open or open and forward. Pressures created by stretch of the muscles and soft tissues are transmitted to the dental and skeletal structures, moving teeth and modifying growth. The monobloc developed by Robin in the early 1900s is generally considered the forerunner of all functional appliances, but the activator developed in Norway by Andresen in the 1920s (Figure 10-2) was the first functional appliance to be widely accepted.
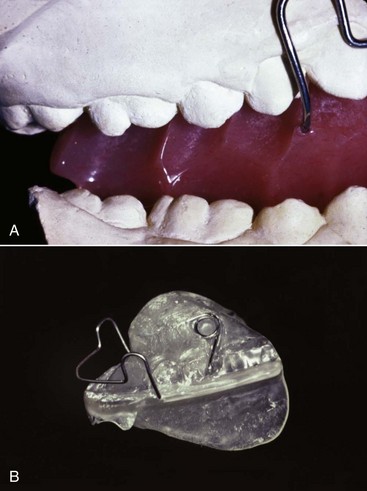
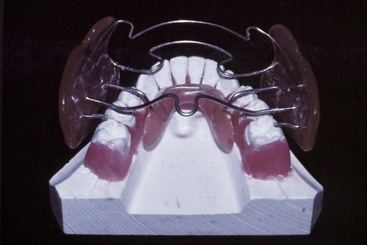
In the European approach at that time, removable appliances often were differentiated into “activators,” or functional appliances aimed at modifying growth, and “active plates” aimed at moving teeth. In addition to the functional appliance pioneers, two European orthodontists deserve special mention for their contributions to removable appliance techniques for moving teeth. Martin Schwarz in Vienna developed and publicized a variety of “split plate” appliances, which were effective for expanding the dental arches (Figure 10-3). Philip Adams in Belfast modified the arrowhead clasp favored by Schwarz into the Adams crib, which became the basis for English removable appliances and is still the most effective clasp for orthodontic purposes (Figure 10-4).

Functional appliances were introduced into American orthodontics in the 1960s through the influence of orthodontic faculty members with a background in Europe (of whom Egil Harvold was prominent) and later from personal contact by a number of American orthodontists with their European counterparts. (Fixed appliances spread to Europe at the same time through similar personal contacts.) A major boost to functional appliance treatment in the United States came from the publication of animal experiment results in the 1970s showing that skeletal changes really could be produced by posturing the mandible to a new position and holding out the possibility that true stimulation of mandibular growth could be achieved (see Chapter 8). Although some of the enthusiasm for functional appliance treatment caused by the favorable animal experiments has faded in the light of less impressive results from clinical trials and retrospective clinical studies (see Chapter 13), functional appliances have achieved a major place in contemporary growth modification treatment.
Modern removable appliance therapy consists largely of the use of (1) various types of functional appliances for growth guidance in adolescents and, less frequently, in children; (2) active plates for tooth movement, used primarily in preadolescents; and (3) clear plastic aligners for tooth movement in adults. The focus of this part of the chapter, accordingly, is on the characteristics of the appliances used for these purposes, especially clear aligner therapy (CAT) for comprehensive treatment in adults and older adolescents. Clinical use of removable appliances in mixed dentition treatment is covered in Chapters 11 and 13, and the application of clear aligner therapy to specific problems in adults is discussed in Chapter 18.
Functional Appliances for Growth Modification
The design and fabrication of many types of functional appliances are covered in detail in a text devoted to the subject.1 The goal here is to put these devices in a contemporary perspective. All are used for growth modification in preadolescents and adolescents, and all are fabricated from a construction bite that advances the mandible in Class II patients and rotates it downward in Class III patients. Bite blocks for anterior teeth are used in short-face/deep-bite patients, and bite blocks for posterior teeth are used in long-face/open-bite patients.
Functional appliances are understood best when viewed as falling into one of four broad categories:
1 Passive Tooth-Borne
These appliances have no intrinsic force-generating capacity from springs or screws and depend only on soft tissue stretch and muscular activity to produce treatment effects. In current use, the bionator (Figure 10-5), twin block (Figure 10-6), and Herbst appliances (Figure 10-7) are examples of passive tooth-borne appliances. The bionator is always removable, the twin block usually is removable but can be fixed, and the Herbst appliance usually is fixed but can be made to be removable.

3 Tissue-Borne
The Frankel appliance (which Frankel called the function regulator) is the only tissue-borne functional appliance (Figure 10-8). Insofar as possible, contact of the appliance with the teeth is avoided. Much of the appliance is located in the vestibule, holding the lips and cheeks away from the dentition. This makes it an arch expansion appliance in addition to its effects on jaw growth because the arches tend to expand when lip and cheek pressure is removed.
4 Hybrid
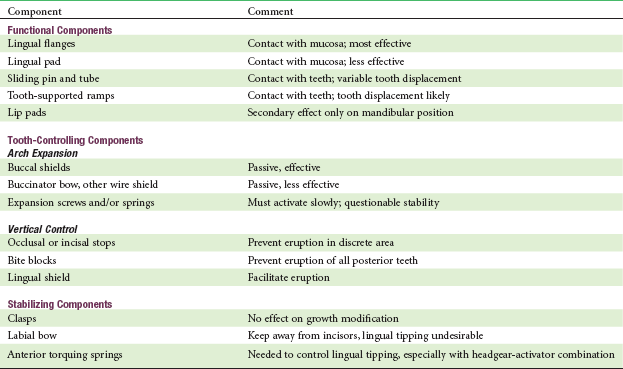
Hybrid functionals are composed of components that are common to functional appliances but are combined to meet a specific need, often in the treatment of jaw asymmetry (Figure 10-9). The components of functional appliances are shown in Table 10-1. They can be combined as needed for individual patients.
Functional appliances are used primarily in late preadolescent children and during the adolescent growth spurt. They are discussed in more detail in Chapter 13.
Removable Appliances for Tooth Movement in Children
Active Plates for Arch Expansion
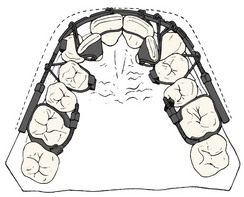
The framework of an active plate is a baseplate that serves as a base in which screws or springs are embedded and to which clasps are attached. The active element usually is a jackscrew placed so that it holds the parts of the plate together (see Figure 10-3). Opening the screw with a key then separates the sections of the plate. The screw offers the advantage that the amount of movement can be controlled, and the baseplate remains rigid despite being cut into two parts. The disadvantage is that the force system is very different from the ideal one for moving teeth. Rather than providing a light but continuous force, activation of the screw produces a heavy force that decays rapidly. Activating the screw too rapidly results in the appliance being progressively displaced away from the teeth rather than the arch being expanded as desired.
Removable Appliances with Springs for Tooth Movement
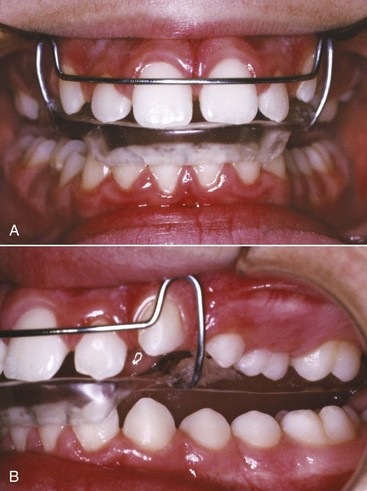
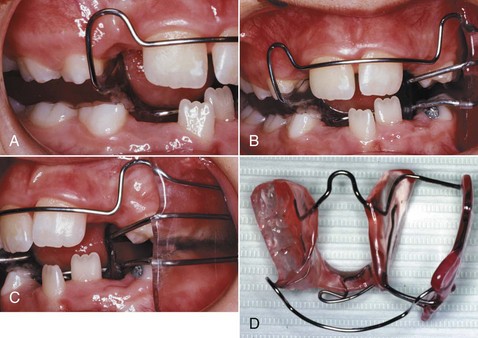
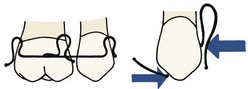
In contrast to the heavy, rapidly decaying forces produced by a screw, nearly optimum light continuous forces can be produced by springs in a removable appliance. Like the edges of an active plate, however, these springs contact the tooth surface at only one point, and it is difficult to use them for anything but tipping tooth movements (although this is theoretically possible) (Figure 10-10). The guideline for tooth movement with a spring from a removable appliance therefore is that this approach should be used only when a few millimeters of tipping movement is acceptable.
Because these appliances are used primarily for minor tooth movement in children, they are discussed in more detail in Chapters 11 and 12.
Clear Aligner Therapy
The use of clear aligners in orthodontic treatment for adults became possible as vacuum-formed clear thermoplastic sheets were introduced into orthodontics in the 1980s. These “suck-down” materials were used initially as retainers and still are important for this purpose (see Chapter 17). It became apparent rather quickly, however, that if teeth were reset slightly and the vacuum-formed sheet was made to fit the reset teeth, a tooth moving device rather than a retainer would be the result. The device now could be, and quickly was, called an “aligner” because the typical use was to bring mildly displaced teeth back into alignment, as, for instance, when mild irregularity of maxillary or mandibular incisors occurred in an orthodontic patient after retainers were discontinued.
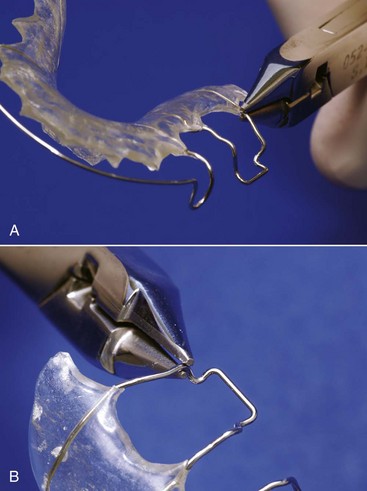
Only small amounts of tooth movement are possible with a single aligner, however, because of the stiffness of the plastic material. To obtain more than minor changes, it was necessary either to reshape the aligner or make a new one on a new cast with the teeth reset to a greater degree. Because the suck-down material is softened and becomes moldable when heated, it would be possible to alter the shape of an aligner with a heated instrument,2 and in an attempt to extend the use of aligners, a special heated pliers for this type of reshaping was offered as a way to avoid the cost and complexity of having to make multiple new aligners (Figure 10-11). This still allowed only minor tooth movement, and skill was required to obtain just the right amount of change in the aligner. A major limitation is that the plastic can only be stretched a maximum of about 3 mm (in 1 mm increments) before it becomes too thin to exert force. More recently, hard plastic bumps that snap into a hole in the aligner have been used to modify it for further tooth movement, which has the advantage that the plastic of the aligner is not stretched and thinned.3

This new approach was introduced with television publicity for “Invisalign” that was designed to create consumer interest in this new approach. The early days of Invisalign treatment were wrought with problems because staging of treatment, optimal rates of tooth movement, and indications for use of attachments on the teeth had not been worked out, and initial professional acceptance of the method was spotty. The technique has matured, however, as clinical evaluation has clarified the best sequence of steps in treatment and the amount of tooth movement in steps that should be attempted, and as the use of tooth-colored shapes bonded to the teeth has improved the appliance’s grip on the teeth and ability to move them. Although remarkably little has been published about the outcomes of Invisalign treatment, there is no doubt now that for many adults, complex malocclusions can be successfully treated in this way (see Chapter 18). As patents expire or are challenged successfully, it is likely that competitive companies will offer sequenced aligners based on modifications of the current techniques.
Invisalign Production Process
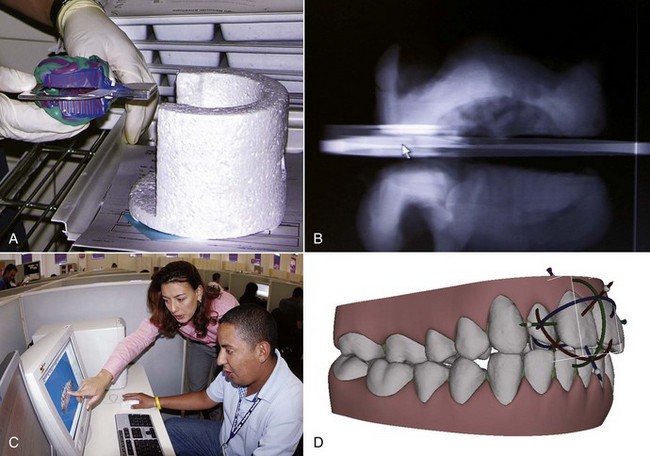
Steps in Preparing the Aligners: Diagnostic records for CAT are not different from those for any other type of orthodontic treatment, but for Invisalign sequenced aligners, an intraoral optical scan (which also records the initial set of the patient’s bite) or PVS (polyvinyl siloxane) impressions and a bite registration (maximum intercuspation) are obtained. The scan or impressions and photographs are submitted to the company along with the doctor’s initial instructions. The production process begins when the intraoral scan or impressions are used to create an accurate three-dimensional (3-D) digital model of each dental arch (Figure 10-12). These records are transferred electronically to a digital treatment facility (presently in Costa Rica).
At the digital treatment facility, the teeth are digitally sectioned and cleaned up (obvious artifacts removed), the dental arches are related to each other, gingiva is added, movement is staged following the doctor’s instructions, and this preliminary plan is placed online for the doctor’s review as a “ClinCheck.” After the doctor is satisfied with the planned sequence of aligners, the set of digital models for a patient is transferred to a cast production facility, where a stereolithographic model for each step is fabricated (Figure 10-13). A clear plastic aligner is formed over each model, and the set of aligners is sent directly to the doctor.

Clinician’s Role in ClinCheck: With experience, doctors tend to be more specific in their initial prescription of what they want, but the sequence of steps and the amount of movement between steps is specified by algorithms built into the Treat software if this is not spelled out in detail in the prescription. In essence, when the ClinCheck is posted for the doctor to examine, the computer technician has sent a draft treatment plan for review (Figure 10-14). The software used by the computer technicians has default scenarios for different types of malocclusions and default rates of tooth movement. These defaults are satisfactory for simpler cases but not for the more complex ones.

For complex treatment, the doctor must customize the plan in terms of the amount and location of interproximal reduction of teeth (if any) that is to be done (Figure 10-15), the sequence of tooth movement steps, the rate of tooth movement with each subsequent aligner (often reducing the amount of movement at critical points), and the extent to which bonded shapes are to be used to increase the aligner’s grip on the teeth.
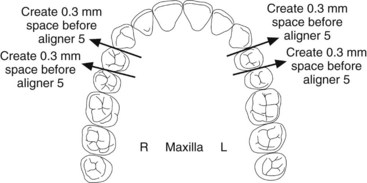
FIGURE 10-15 The Invisalign reproximation form (same patient as Figure 10-14), specifying how much enamel is to be removed from teeth and when in the sequence of aligners the reproximation will be done. For this patient, the upper incisors are to be reduced slightly in width to facilitate their alignment.
Considerations in Clinical Use of Clear Aligners: Although Invisalign is over a decade old, only a few studies of the outcomes of Invisalign treatment have been published in refereed professional journals.4 A recent prospective study used Invisalign’s software to evaluate the accuracy with which planned changes were accomplished, using the ratio of achieved to predicted change, and found that the highest accuracy (47%) was achieved during lingual constriction of the dental arches and the lowest (18%) for extrusion of maxillary incisors.4 Based on the existing studies and comments from experienced users, it seems clear now that Invisalign (and clear aligners more generally) do some things well and others not so well (Box 10-1). The limitations should be kept in mind when CAT is considered.
Several other considerations in the use of sequential aligners include the following:
• The use of attachments that are bonded to selected teeth greatly extends the possible tooth movement with aligners. In general, significant root movement (as in the closure of extraction sites) is almost impossible without the use of attachments, as is closure of open bites by elongation of incisor teeth; with attachments, both are possible (see Figures 18-40 and 18-41). Even with attachments, significant rotation of rounded teeth (canines and premolars) is difficult. It is possible to bond a button to a rotated tooth so that a rubber band can be used to rotate it while an aligner is being worn (see Figure 10-14). There is an increasing trend toward a combination approach to complex treatment, using a short phase of partial fixed appliances or auxiliaries in addition to the sequence of aligners.
• Interproximal enamel reduction (IPR) to obtain space for aligning crowded teeth often is part of the treatment plan. If IPR is planned, removal of interproximal enamel in the canine-premolar region to provide space can be used in addition to reduction in the width of incisors. The amount of interproximal reduction is part of the doctor’s prescription (see Figure 10-15).
• Patients must be monitored carefully to verify that tooth movement is tracking with the series of aligners (i.e., that all teeth are seated completely in the aligner after it has been worn for the specified period of time). If the teeth are not tracking, there are several possibilities: not enough wear of the aligners by the patient, insufficient interproximal reduction, insufficient crown height or shape to allow a grip on the tooth or teeth to be moved, wrong type or position of bonded attachments, or movement created in ClinCheck that is too fast to be possible biologically. A refinement or midcourse correction, with a new intraoral scan or PVS impressions and revision of the treatment plan, often is necessary in treatment of complex problems.
• Aligners cover the teeth like a bleaching tray, and they can be used to bleach during treatment (unless the patient has bonded attachments on the anterior teeth). If this is done, it is important to remember that tooth movement causes transient pulpitis and so does bleaching. The combination of the two procedures can lead to significant tooth sensitivity. This can be controlled by increasing the intervals between bleaching sessions, but bleaching usually is better deferred until the retention stage.
The clinical use of clear aligners in adjunctive and comprehensive treatment is discussed in greater detail in Chapter 18.
Fixed Appliances
The Development of Contemporary Fixed Appliances
Angle’s Progression to the Edgewise Appliance
E-Arch: In the late 1800s, a typical orthodontic appliance depended on some sort of rigid framework to which the teeth were tied so that they could be expanded to the arch form dictated by the appliance. Angle’s first appliance, the E-arch, was an improvement on this basic design (Figure 10-16). Bands were placed only on molar teeth, and a heavy labial archwire extended around the arch. The end of the wire was threaded, and a small nut placed on the threaded portion of the arch allowed the archwire to be advanced so that the arch perimeter increased. Individual teeth were simply ligated to this expansion arch. This appliance still could be found in the catalogs of some mail-order orthodontic laboratories as late as the 1980s, perhaps because of its simplicity, and despite the fact that it can deliver only heavy interrupted force.
Pin and Tube: The E-arch was capable only of tipping teeth to a new position. It was not able to precisely position any individual tooth. To overcome this difficulty, Angle began placing bands on other teeth and used a vertical tube on each tooth into which a soldered pin from a smaller archwire was placed. With this appliance, tooth movement was accomplished by repositioning the individual pins at each appointment.
Ribbon Arch: Angle’s next appliance modified the tube on each tooth to provide a vertically positioned rectangular slot behind the tube. A ribbon archwire of 10 × 20 gold wire was placed into the vertical slot and held with pins (Figure 10-17). The ribbon arch was an immediate success, primarily because the archwire, unlike any of its predecessors, was small enough to have good spring qualities and therefore was quite efficient in aligning malposed teeth. Although the ribbon arch could be twisted as it was inserted into its slot, the major weakness of the appliance was that it provided relatively poor control of root position. The resiliency of the ribbon archwire simply did not allow generation of the moments necessary to torque roots to a new position.
Edgewise: To overcome the deficiencies of the ribbon arch, Angle reoriented the slot from vertical to horizontal and inserted a rectangular wire rotated 90 degrees to the orientation it had with the ribbon arch, thus the name “edgewise” (Figure 10-18). The dimensions of the slot were altered to 22 × 28 mils, and a 22 × 28 precious metal wire was used. These dimensions, arrived at after extensive experimentation, did allow excellent control of crown and root position in all three planes of space.
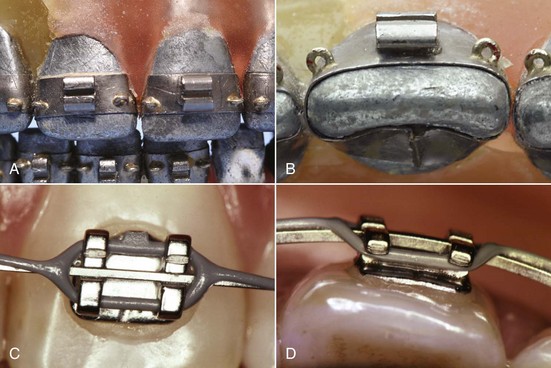
FIGURE 10-18 A and B, Angle’s edgewise appliance received its name because the archwire was inserted at a 90-degree angle to the plane of insertion of the ribbon arch, which made it wider than it was tall. The rectangular wire could be twisted to create torque (see Figure 10-22). It was tied into a rectangular slot with wire ligatures, making excellent control of root position possible. The original appliance is seen here on a typodont. Note the narrow brackets (double width on the maxillary centrals, which are wider teeth), which were soldered to gold bands. Also note the eyelets soldered on the corners of the bands. These were used for ligature ties to the archwire as needed for rotational control. C and D, Close-up views of a modern edgewise twin bracket with a rectangular archwire in place. The wire is held in the bracket by an elastomeric ligature, here part of a chain of ligatures that also keep spaces closed between the teeth.
Other Early Fixed Appliance Systems
Labiolingual, Twin Wire: Before Angle, placing attachments on individual teeth simply had not been done, and Angle’s concern about precisely positioning each tooth was not widely shared during his lifetime. In addition to a variety of removable appliances utilizing fingersprings for repositioning teeth, the major competing appliance systems of the first half of the twentieth century were the labiolingual appliance, which used bands on first molars and a combination of heavy lingual and labial archwires to which fingersprings were soldered to move individual teeth, and the twin-wire appliance. This appliance used bands on incisors as well as molars and featured twin 10 mil steel archwires for alignment of the incisor teeth. These delicate wires were protected by long tubes that extended forward from the molars to the vicinity of the canines. None of these appliances, however, were capable of more than tipping movements except with special and unusual modifications. They have disappeared from contemporary use.
Begg Appliance: Given Angle’s insistence on expansion of the arches rather than extraction to deal with crowding problems, it is ironic that the edgewise appliance finally provided the control of root position necessary for successful extraction treatment. The appliance was being used for this purpose within a few years of its introduction. Charles Tweed, one of Angle’s last students, was the leader in the United States in adapting the edgewise appliance for extraction treatment. In fact, little adaptation of the appliance was needed. Tweed moved the teeth bodily and used the subdivision approach for anchorage control, first sliding the canines distally along the archwire, then retracting the incisors (see Figure 9-33).
Begg’s adaptation took three forms: (1) he replaced the precious metal ribbon arch with high-strength 16 mil round stainless steel wire as this became available from an Australian company in the late 1930s; (2) he retained the original ribbon arch bracket, but turned it upside down so that the bracket slot pointed gingivally rather than occlusally; and (3) he added auxiliary springs to the appliance for control of root position. In the resulting Begg appliance (Figure 10-19),5 friction was minimized because the area of contact between the narrow ribbon arch bracket and the archwire was very small and the force of the wire against the bracket was also small. Binding was minimized because Begg’s strategy for anchorage control was tipping/uprighting (see Figure 8-21), and tipping minimizes the angle of contact between the wire and corner of the bracket.

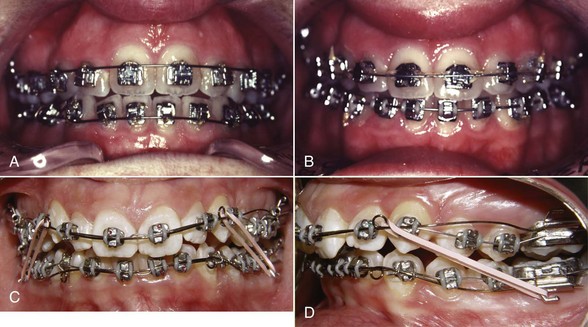
Although the progress records with his approach looked vastly different, it is not surprising that Begg’s overall result in anchorage control was similar to Tweed’s, since both used two steps to compensate for resistance to sliding. The Begg appliance is still seen in contemporary use though it has declined in popularity and often appears now in a hybrid form, with brackets that allow the use of rectangular wires in finishing (Figure 10-20).6 It is a complete appliance in the sense that it allows good control of crown and root position in all three planes of space.
Contemporary Edgewise
Automatic Rotational Control: In the original appliance, Angle soldered eyelets to the corners of the bands, so a separate ligature tie could be used as needed to correct rotations or control the tendency for a tooth to rotate as it was moved (see Figure 10-18). Now rotation control is achieved without the necessity for an additional ligature by using either twin brackets or single brackets with extension wings that contact the underside of the archwire (Lewis or Lang brackets) (Figure 10-21) to make it easier to obtain the necessary moment in the rotational plane of space.

Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


