CHAPTER 14
Class III Correctors
The skeletal Class III malocclusion is characterized by mandibular prognathism, maxillary deficiency, or a combination of both. These patients may have a retrusive nasomaxillary area and a prominent lower third of the face. Intraorally, patients usually present with a Class III molar relationship and a reverse overjet depending on the severity of the skeletal discrepancy.
Many treatment approaches have been advocated for Class III patients, ranging from early orthopedic intervention to camouflage and definitive surgical intervention. Methods designed to intercept the developing malocclusion have included maxillary expansion and protraction with a facemask, chin cup and fixed orthodontic appliance therapy. In this chapter, an attempt is made to answer a few frequently asked questions related to the use of these Class III correctors, including the indications for treatment, treatment timing, and the response of these appliances to treatment.
1 What is pseudo Class III malocclusion, and how can these patients benefit from early treatment?
Patients with pseudo Class III malocclusion often present with anterior crossbites that are caused by a premature tooth contact or improper inclinations of the maxillary and mandibular incisors (< ?xml:namespace prefix = "mbp" />

FIG 14-1 A-C, Patients with a pseudo Class III malocclusion can often present with an anterior crossbite (A and B) that can be manipulated back to an end-to-end incisal relationship in centric relation (C).
Correction of single or multiple anterior teeth in crossbite can be accomplished by using a fixed or removable appliance with an inclined plane, removable appliance with auxiliary spring, and lingual arch with finger springs (

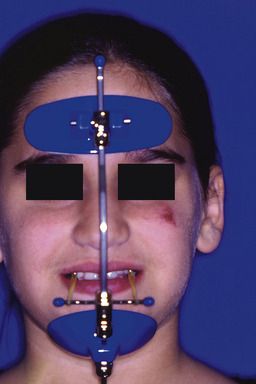
2 What is a Delaire facemask?
The Delaire protraction facemask is used in the treatment of patients with Class III malocclusion and a maxillary deficiency.
The protraction facemask is made of two pads that contact the soft tissue in the forehead and chin region (
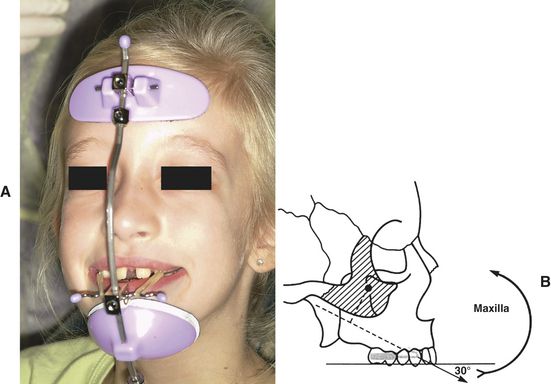
3 When is facemask therapy indicated?
The facemask is most effective in the treatment of mild to moderate skeletal Class III malocclusions with a retrusive maxilla and a hypodivergent growth pattern. Patients presenting with some degree of anterior mandibular shift on closure and a moderate overbite have a more favorable prognosis (
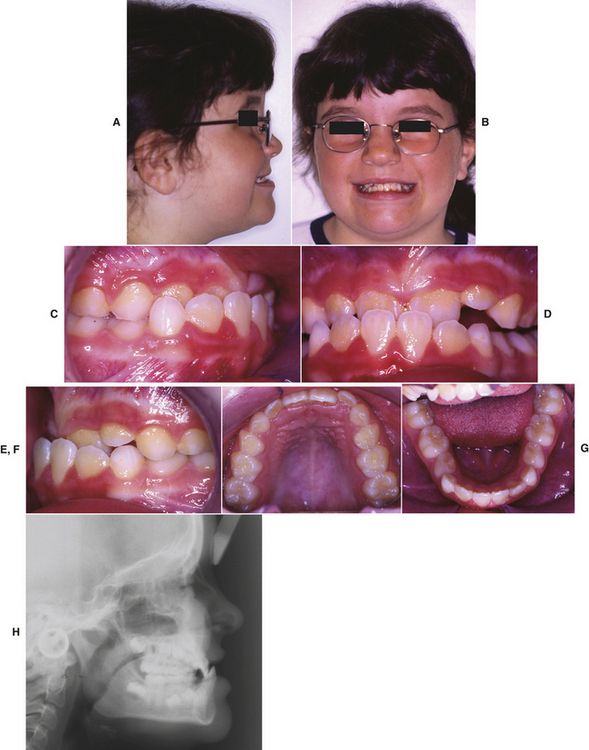

FIG 14-5 A-H, Eight-year-old patient with a Class III malocclusion and a deficient maxilla treated with maxillary expansion and protraction. A and B, Facial photos. C-G, Intraoral photos.H, Cephalometric radiograph. I-P, Posttreatment photographs showing an improvement in facial profile and correction of the anterior crossbite with 8 months of maxillary protraction. I and J, Facial photos. K-O, Intraoral photos. P, Cephalometric radiograph.
4 Is expansion necessary for protraction facemask treatment?
Various appliances have been used as anchorage for maxillary protraction, including palatal arches and banded and bonded expansion appliances (
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


