CHAPTER 10
Treatment Tactics for Problems Related to Dentofacial Discrepancies in Three Planes of Space
All orthodontic appliances produce both desired and undesired tooth movements. The science and art of orthodontics is to balance forces in order to maximize the desired movement and minimize the undesired movement. This balance is achieved through proper decision making in three areas: (1) appliance selection, (2) appliance utilization, and (3) timing of appliance therapy.
Appliance selection is critical for successful treatment outcomes. For instance, when selecting a functional appliance, one has to consider that certain functional appliances may lead to undesirably procumbent lower incisors. Proper appliance utilization is critical for minimizing undesired tooth movements, such as flaring of the lower incisors. If lower incisor flaring is a concern, a tissue-borne functional appliance or a tooth-born appliance such as a MARA used in conjunction with fixed appliances using a full-size lower archwire can minimize lower incisor flaring. In addition, the use of Class II elastics without establishing proper anchorage may lead to extrusion of posterior teeth, anterior open bite, and excessive tipping of the occlusal plane.
Although proper appliance selection and utilization are two critical issues in effective orthodontic treatment, successful treatment outcomes may not be achieved without appropriate timing of appliance therapy. Using an orthodontic appliance at an inappropriate time may lead to ineffective treatment and result in undesired tooth movements. For example, the use of a rapid palatal expander (RPE) in a skeletally mature patient may cause excessive tipping of posterior teeth, lingual cusp interferences, anterior open bite, adverse periodontal consequences, and high potential for orthodontic relapse after treatment. Timing of appliance therapy also relates to the sequence of treatment events. Attempting space closure and anterior tooth retraction without proper anchorage preparation may lead to undesired tooth movements that cannot be reversed. Consequently, selection, utilization, and timing of appliance therapy are intertwined and involve a comprehension of tooth movement in the transverse, vertical, and anterior-posterior dimensions.
TRANSVERSE DISCREPANCIES
1 Under what circumstances should a maxillary expansion appliance be used?
2. What are the different types of expansion appliances?
BANDED EXPANDERS
Hyrax Expander
The Hyrax expander consists of two bands on the upper first molars and usually two bands on the upper first bicuspids (
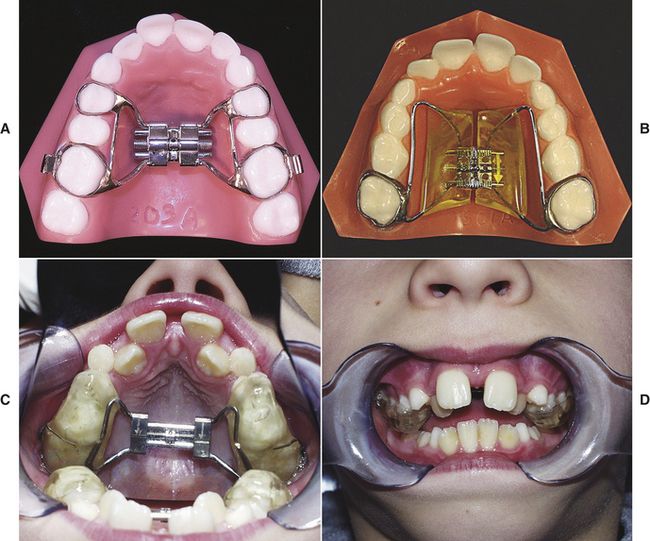
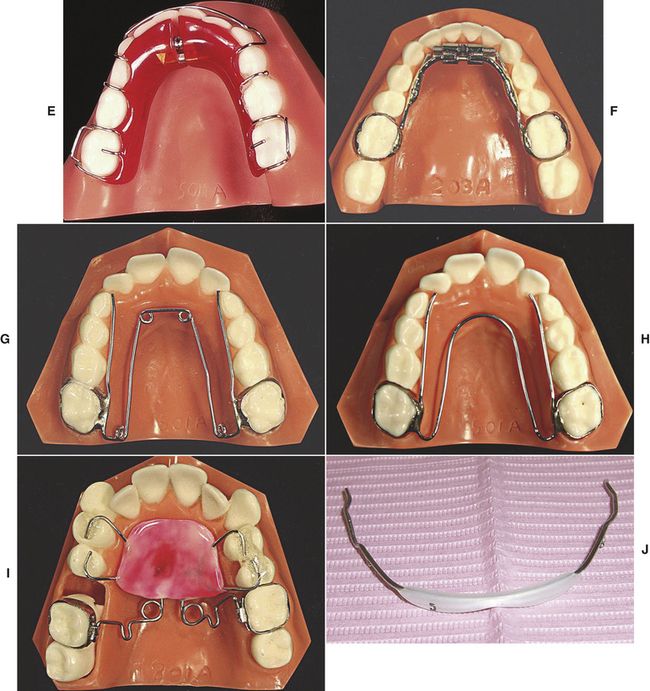
FIG 10-1 A, The Hyrax maxillary expander. B, The Haas maxillary expander. C and D, The bonded rapid palatal expander: palatal view (C) and frontal view (D). E, Removable Schwartz appliance. F, Fixed mandibular expander. G, Quadhelix. H, W arch. I, Pendex appliance. J, Lip bumper appliance.
(A, B, E-I, courtesy AOA Orthodontic Appliances, Sturtevant, Wisc.)
Haas Expander
The Haas expander is a fixed maxillary expander that uses acrylic pads and heavy lingual wires to apply pressure to both the teeth and the palatal tissue during expansion. This expander is thought to result in less tipping of the buccal tooth segments (
BONDED RAPID PALATAL EXPANDER
Bonded RPE is an alternative to the banded design. It is a fixed appliance that uses posterior acrylic coverage and is directly bonded to the teeth (
LOWER SCHWARTZ APPLIANCE (REMOVABLE)
Lower Schwarz appliance (
FIXED MANDIBULAR EXPANDER
Fixed mandibular expander is used as an alternative to the removable Schwarz appliance. This fixed metal expander provides lateral expansion in the mandibular arch (
QUADHELIX
This fixed metal expander is capable of applying forces in numerous directions depending upon how it is activated by the orthodontist (
W ARCH
W arch is similar to the quadhelix without the four helical loops (
PENDEX
Pendex is a fixed expansion appliance that is also used to distalize and derotate one or both upper first molars (
LIP BUMPER
A lip bumper (
CONVENTIONAL FIXED APPLIANCES
Arch wires can be expanded transversely to achieve dental expansion in either the maxilla or mandible.
3 Which expansion appliance should I use?
Factors that influence the selection of an expansion appliance include, but are not limited to, patient’s age or skeletal maturity, the clinician’s desire for dental versus skeletal expansion, the number of teeth available for anchorage, the expectation for patient compliance, and whether the expander will be used in conjunction with fixed appliances or other appliances, such as a facemask.
4 When should expansion be initiated?
Treatment of crossbite with a functional shift should be initiated as soon as it is diagnosed. If not treated, these crossbites may adversely affect growth. If the mandible shifts to one side, growth will be asymmetric and the chin will deviate to that side. Also, very narrow upper arches should be treated as early as possible. As the patient matures, it is hard to get skeletal expansion. These narrow upper arches are usually associated with significant crowding and are best corrected when the patient is skeletally immature. Expansion in skeletally mature patients may result in undesired dental movement; therefore, the best time to correct these constricted arches is usually in the mixed dentition.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


