1
Anomalies of Number
1.1 Introduction
The human dentition may consist of fewer or more than the normal number of 20 deciduous or 32 permanent teeth. Fusion of two teeth may also give the impression of hypodontia (Section 1.2).
1.2 Hypodontia
Hypodontia is the term used for dentitions with fewer than the regular number of teeth due to agenesis, i.e. either absence of a tooth germ or failure of a tooth germ to develop. Anodontia is the congenital absence of all the teeth while the absence of many teeth is known as oligodontia or partial anodontia. Isolated hypodontia is the congenital absence of one or a few teeth. Incomplete dentitions not classified as having hypodontia by definition are those where teeth are absent due to failure of eruption, extraction due to caries or orthodontic treatment,295 or where teeth have been lost due to trauma and other reasons.
Hypodontia is the most frequent of all congenital aberrations in humans, and also occurs in animals such as dogs.245 The incidence of agenetic teeth in Caucasian populations seems to have increased during the twentieth century, but the available data are too limited to suggest a trend.384
The aetiology of hypodontia is not entirely clear, but genetic factors are most certainly involved. Because mutated genes associated with agenesis have developmental regulatory functions elsewhere in the embryo, associated defects in other tissues and organs are also possible.591
The skin develops from the ectoderm, one of the three primary germ layers, which is involved in the formation of the teeth. Patients with isolated dental agenesis may show unusual dermatoglyphic patterns of the palms of the hands and soles of the feet, suggesting a shared origin.28 The combination of freckles, thin eyebrows and hypodontia609 suggests the same. Therefore, isolated dental agenesis might be a minor manifestation of a systemic disorder.
1.2.1 Isolated Dental Agenesis
As mentioned above, isolated dental agenesis is the result of the absence of one or a few tooth germ(s). Missing teeth can lead to diastema (interdental spaces) in the dental arches. Displacement and tilting of the neighbouring teeth may close these spaces.
Epidemiology
Primary Dentition
Less than 1% of children exhibit hypodontia in the deciduous dentition. The teeth most often involved are the maxillary incisors, followed by the mandibular central or lateral incisors,112 134 220 372 394 445 469 and also the first molars.112 When the deciduous canines are agenetic, 205 608 a syndrome (see Chapter 11) such as cleft lip is usually present.464 Around 50% of children with hypodontia are missing one tooth, usually the maxillary lateral incisor; in the rest usually two or more teeth are missing.134 Japanese children show agenesis more frequently (5%), which may represent an ethnic trait.112 158
Permanent Dentition
Surveys, often retrospective, of some 160 000 children and adolescents from different countries and populations indicate that 2% to 10% of the permanent dentitions show isolated dental agenesis, third molars excepted.1 10 31 47 55 89 94 112 129 131 159 169 170 208 210 219 231 268 279 294 352 362 371 374 388 410 414 421 423 441 469 485 488 508 541 594 595 629 638 648 One study found that 13% of orthodontic patients had hypodontia,476 however, this sample is not representative of the population and the finding may be considered as an outlier.
The main body of data has been collected from European and American Caucasian populations, although some studies have included different ethnic and mixed populations. European and Australian children in general lack more teeth than North American Caucasians.446 On average two teeth, frequently homologous teeth,31 per individual are agenetic.160
Girls are significantly more susceptible to agenesis than boys,1 31 47 169 200 219 279 476 485 488 452 566 664 but not all surveys have found a difference between the sexes. 159 374 497 501 574 665 Isolated dental agenesis may, however, occur about 1.4 times more often in girls than boys,384 446 and agenesis of several teeth is also more common in girls.210 585 595 In one study, the prevalence of hypodontia in Jewish children did not differ by sex, but girls lacked the maxillary lateral incisors more frequently and the boys the mandibular incisors.170
The overall prevalence of agenesis in the maxilla is comparable with that in the mandible, but there is a marked difference in the pattern of absence of tooth type between the jaws.446 The five teeth most prone to agenesis in order of most to least prevalent, are: third molars > mandibular second premolars > maxillary lateral incisors > maxillary second premolars > mandibular lateral incisors.
However, other rank orders of agenesis of teeth, including teeth other than the ones mentioned above, have also been reported. Specific populations and inclusion of oligodont patients may account for the differences.446
Third Molars
Wisdom teeth are most often implicated in isolated dental agenesis, but the prevalence data vary. In 10–35% of adolescent and young adult dentitions, one to four third molars are absent.5 33 34 73 129 200 231 234 250 260 255 276 308 412 441 455 511 535 554 594 596 In studies of third molar agenesis, subjects may not be very young since the teeth develop quite late in some individuals,61 474 and older people may not recollect whether the teeth were extracted.
Third molar agenesis seems race-related.33 132 260 524 554 For instance, 27% of the white population in the USA versus 2% of East Africans have missing wisdom teeth,33 and more Chinese lack all four third molars than Caucasians.132 Women lack wisdom teeth less often than men,444 but some researchers did not find a sex difference.346 354
More so than other teeth, the third molars tends to show bilateral absence.129 354 554 Almost 10% of subjects also lack other teeth when one or more third molars are agenetic.73
Mandibular Second Premolar
Of the four frequently agenetic teeth (excluding third molars), 45% or more47 466 are second mandibular premolars; they are bilaterally missing in almost half of the population missing these teeth.574 The reported percentages for lower second premolar agenesis vary considerably, but may be as low as 3.5%. In some studies, the maxillary lateral incisors were the most frequently agenetic,55 170 410 501 580 638 and in one study it was the mandibular lateral incisors.131 Such variations in findings might be due to ethnic differences.444 524 Studies in Caucasians are more likely to show absence of the mandibular second premolar (and maxillary lateral incisor), and Asian studies of the mandibular incisors. A difference between the sexes has not been established.574
Maxillary Lateral Incisor
A quarter of the four most frequently agenetic teeth (excluding third molars) are the maxillary lateral incisors. In some studies these teeth are reported to be missing even more often than the second mandibular premolars. A meta-analysis showed almost equal rates of agenesis of the maxillary lateral incisors and the maxillary second premolars.384 In about 2.2% of Caucasians and Israelis the maxillary lateral incisor is absent.170 580 Bilateral agenesis is common,446 and the anomaly may be more common in women.566
Figure 1.1 shows a congenitally missing right maxillary lateral incisor and an underdeveloped contralateral incisor, which is rarer than bilateral agenesia.566 The reduced, often conical, morphology may represent an incomplete expression of agenesis.444
Figure 1.1 Agenetic right permanent maxillary lateral incisor; the contralateral tooth is underdeveloped.

Maxillary Second Premolar
This tooth accounts for some 20% of the four frequently agenetic teeth, excluding the third molars. The variations in figures may be ascribed to small sample sizes, but the large differences in reported prevalences is substantial and remains unexplained. Bilateral agenesis occurs thrice as often as unilateral agenesis.444
Mandibular Central Incisor
In order of frequency of agenesis in the permanent teeth, the mandibular central incisors usually come last, but not in Chinese children in Hong Kong.131 Occasionally, the lateral incisor has been found to be missing more often than the central. Figures 1.2 and 1.3 show two and four retained deciduous mandibular incisors, respectively, due to absence of their successors.
Figure 1.2 Agenetic permanent central incisors – the deciduous teeth are retained.
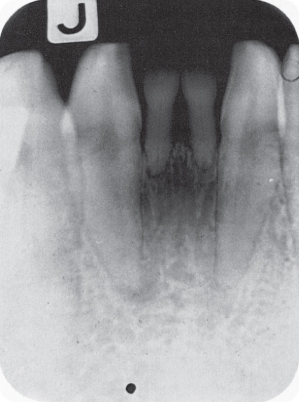
Figure 1.3 Four retained deciduous incisors in the mandible; the permanent successors are agenetic.

Other Teeth
Any other tooth may be agenetic, and this is termed “aplasia of atypical elements”.524 For instance, absence of the maxillary first premolar,159 second molar47 166 279 410 and the mandibular first premolar has been reported.47 210 When the first permanent molar does not develop, other teeth tend to be missing too (oligodontia).230 289 344 The maxillary central incisors are almost always present,541 the canines being more often agenetic.524 The condition in which there is presence of just one central incisor is described in Section 1.4.
Aetiology
Agenesis of teeth has been attributed to infectious diseases such as rubella, birth trauma, endocrine disorders, evolution and heredity.268 572 For instance, one mother and her three daughters all had congenitally missing mandibular incisors, albeit different ones.415
Evolution
The relationship between agenesis and evolutionary processes is not clear.
Human teeth are diphyodont (two generation), except the permanent molars, which are monophyodont.140 The last element of each tooth class (the third molars, second premolars and lateral incisors) is often agenetic or reduced in size. Bolk (1866–1930) therefore proposed the “terminal reduction theory”: that is, during evolution, the distal element in each tooth class tends to disappear. However, of the four archetypal premolars per quadrant, the third and fourth premolars are present in the dentition of modern humans. The third molars would also have disappeared, but the primary fourth molar became the permanent first molar, accounting for the presence of three molars in modern humans.524 628 Bolk’s theory was eventually rejected but is summarised in Table 1.1, which also illustrates the current point of view.
Bolk also postulated that the teeth lost through evolution occasionally re-emerge in Homo sapiens. For instance, the lost lateral incisor reappears as an “additional tooth” between the central incisors (see Section 1.3).
Table 1.1 Teeth per quadrant of the archetypal permanent dentition, the teeth remaining in modern humans according to Bolk, and present point of view628

Heredity
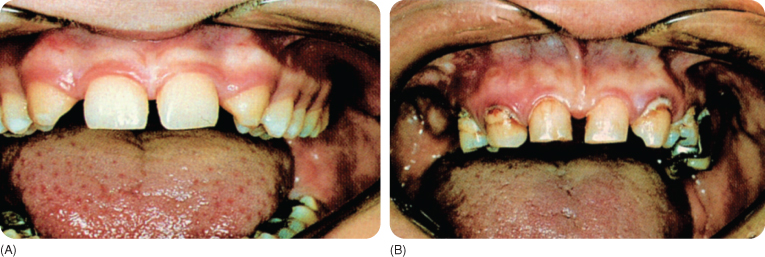
Hypodontia is usually a manifestation of an inherited trait (Figure 1.4) although it can occur sporadically, when it represents an acquired anomaly.619 It is conceivable that certain mutated genes cause hypodontia.591 Hypodontia follows an autosomal dominant mode of inheritance, but incomplete penetrance suggests interference of suppressor genes with the phenotypic expression.92 Research has focused in particular on the maxillary lateral incisors, and, to a lesser degree, the premolars.
- Agenesis of maxillary lateral incisors is an autosomal dominant trait,19 219 376 but other modes of inheritance have also been reported.19 284 413
- Agenesis of premolars is an autosomal dominant trait, with a complete penetrance, but varying expression.577
- Agenesis in particular affects the second premolars together with the lateral maxillary incisors, called the “incisor-premolar trait”, with a penetrance of 86%.284
Figure 1.4 Mother (A) and daughter (B) with agenetic maxillary permanent lateral incisors.
One study found that mutations in the genes for growth factors, which have a regulatory role during odontogenesis, were not responsible for dental agenesis.25 Mutations in more than one gene and possibly multiple alleles are needed to explain the variations in dental agenesis.37 480 488 One proposition is that to become manifest, agenesis must cross a “biological threshold”110 and penetrance would require altered expression of more than one gene. A statistical analysis575 in 171 families185 concluded that hypodontia must be polygenetic.
- The homeobox genes regulate migration of the neural crest cells and tooth morphology. Mutations of the muscle-specific homeobox gene, MSX1, are linked to autosomal dominant agenesis of specific teeth.357 Inactivation of MSX1 has a highly selective effect on the dentition, but other genes must be involved for hypodontia to occur.516 MSX1 encodes transcription factors expressed in several tissues including the dental mesenchyme. MSX1 mutations might be related to agenesis of premolars and molars.357 626 MSX1 is located on chromosome 4; the locus of Notch2 for third molar agenesis has been mapped to chromosome 3 in mice.422 Multiple genes appear to contribute to interfamilial clinical variations in tooth agenesis.619 Data on hypodontia fitted a polygenic model better than a single major gene model.546 Several independent, defective genes acting alone or in combination, and eventually becoming antagonistic, may lead to a specific pattern of phenotypic agenesis.625
- Environmental factors are also implicated. Exposure in childhood to dioxin after an accident in a chemical factory (Seveso, Italy) resulted in increased incidence of hypodontia.9 The association between different cleft types and hypodontia in twins was found to have a weak genetic component,339 possibly because of the small sample size and the presence of environmental factors.
- Confounding factors also exist. Monozygotic twins, born from one fertilised egg, are in principle, genetically identical, but showed differential expression of hypodontia,222 315 403 as mirrored agenesis of mandibular second premolars.345 Regardless of tooth group concordance, mono- and dizygotic twins (born from two fertilised eggs) have similar prevalence rates of bilateral agenetic teeth.64
Dizygotic twins are no more similar than siblings. In the past, matched tooth anomalies were used as determinants of di- and monozygosity,604 but cleavage of the egg can take place in the two-cell stage or later.521 Monozygotic twins may have an abnormal number of (parts of) chromosomes.560 Differing chromosomal compositions may exist through gene mutation or post-zygotic (partial) loss of a chromosome in one twin DNA (copy errors), while the other maintains the karyotype of the zygote. It has been established that monozygotic twins show mirror-image tooth anomalies but discordant hypodontia222 244 312 339 345 403 604 and other dental features.41 52 99 603 604 Moreover, lyonisation is a possibility in monozygotic female twins.
When multiple teeth are agenetic, associated deviant skeleto-dental patterns, such as a retruded maxilla,45 have been hypothesised to be due to environmental effects. Horizontal and vertical pressure on the dental lamina during growth supposedly suppresses or distorts the tooth buds, likely affecting the last tooth in each tooth class.397 One study concluded that in orthodontic patients, the frequency of maxillary and mandibular third molar agenesis is related to a decreased anterior–posterior dimension of solely the maxilla.299
Relationships Between Teeth
In isolated dental agenesis, the teeth that are present show smaller crowns, a “tendency” to agenesis.308 524 A peg maxillary lateral incisor is also associated with non-eruption and a palatally erupted canine.439 440
- Agenesis of the maxillary lateral incisors increases the probability of other teeth being agenetic.349 The same applies to an increasing number of agenetic wisdom teeth.5 201 439 511 554 574 Such relationships are not always present,319 and the reverse has also been reported.491 532
- When the wisdom teeth are agenetic, the anterior teeth in particular may be relatively small, but such findings are not consistent.38 199 497 648
- Agenesis of the maxillary lateral incisor seems to be compensated by a larger adjacent central incisor. When the lateral incisor is undersized, this compensation is not seen; in fact the adjacent central incisor also tends to be relatively small.550
- Agenetic wisdom teeth (in the Inuit) were not found to be associated with a reduced occlusal pattern of the other molars.249
- In at least 50% of patients with a missing deciduous lateral incisor, the successor is agenetic,72 220 290 372 469 and if bilaterally absent, more permanent teeth may be agenetic, such as the rarely involved first and second molars.133
A division of mandibular tooth agenesis into three groups has been suggested, based on the radiological evidence of the mandibular canal. In the anterior part of maxillary jaw, a pronounced lack of teeth was found to be associated with absence or marked reduction in the size of the incisive foramen and nasopalatine canal.320 532
Tooth Germ-Related Causes
For dental agenesis, a tooth germ must be affected during its earliest developmental stages. Likely causes are failure of mesenchyme condensation during the initiation of the tooth bud stage, absence of induction of the subsequent ectodermal reactions and an inability of the ameloblasts to produce enamel following reciprocal induction by the odontoblasts. On combining these tissues in vitro, there was development of tooth-like structures.543 In experimental studies, the formation of the dental papilla was induced in the mandibular epithelial lamina through its contact with non-odontogenic mesenchyme.401
Odontogenesis is initiated in the epithelium and is guided by interactions with the neural crest cells.529 593 Regulation of normal tooth development requires proteins produced by a number of genes for the series of reciprocal interactions between the dental epithelium and mesenchymal condensations, which are accumulations of proliferating cells originating from the neural tube. Some of these cells are pluripotent;77 their absence is related to non-initiation of the tooth germ.390 542
The specific morphology of the teeth is also influenced by the cell condenstations.390 Butler’s “field theory” states that all tooth primordia are initially equivalent and that the morphology of the teeth is determined by morphogenes in the antero–posterior axis.93 Molecular investigations have identified single genes (such as the homeobox genes) with site-specific antero–posterior activity. A defective specific gene has been found to be associated with agenesis of specific posterior teeth, but not the anterior teeth. The developing maxillary dentition is not continuous: the upper incisors develop in the medial nasal processes of the first arch,114 in the premaxilla.
The hypothesis that tooth agenesis is associated with prenatal brainstem anomalies has not been confirmed: the frequency of agenesis in such patients and the population was similar.358
Early disruption of the developmental processes is most probably a result of lack of (reciprocal) signals at the right time,618 due to mutations in genes or an inability of the cells to respond appropriately.
Other Causes
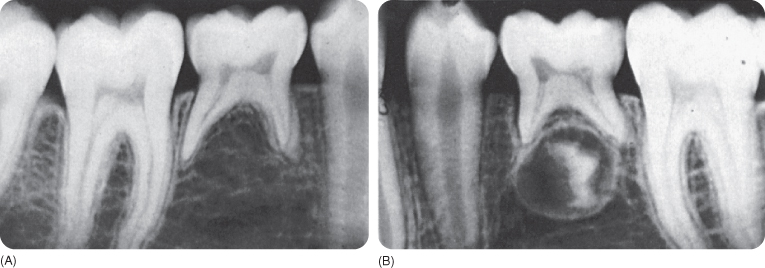
Dental development may be interrupted by diseases such as leprosy or the presence of congenital anomalies involving atrophy or disordered development of the anterior part of the maxilla. Figure 1.5 shows absence of a mandibular second premolar and arrested development of the contralateral tooth.
Figure 1.5 (A) Agenetic lower second premolar with retained deciduous second molar. (B) The development of the contralateral premolar is arrested.
Ionising radiation (radiotherapy) can cause agenesis (and morphologic changes)161 in humans240 217 387 505 and animals84 85 Just one treatment with 15 Gy leads to a temporary interruption in odontogenesis.240 565 After chemotherapy, children showed marked tooth agenesis.16
Segmental odontomaxillary dysplasia is another condition with agenesis of one or both premolars in the affected jaw segment. The disorder consists of a unilateral maxillary enlargement from the canine region to the tuberosity, accompanied by gingival hyperplasia. Superiorly the enlargement occurs at the cost of the maxillary sinus. The spaced deciduous molars may be malformed, with splayed roots and pulp stones in enlarged pulp chambers. If the skin on the affected side contains more sweat glands than normal, the anomaly is called hemi-maxillofacial dysplasia. The cause of the disorder is not known.42 123 162 433 459 622 637
Cutaneous abnormalities, such as “hairy nevus” of the skin and hypopigmentation of the lip border, are less frequently observed.459 637 The anomalies originate in utero or in early childhood. Less common features are enlarged crowns and roots.42 433 The condition seems to remain stable without significant progression.123
Consequences
Consequences of isolated dental agenesis depend on the permanent tooth that is missing.
- When a permanent maxillary lateral incisor is agenetic, the predecessor will exfoliate, because the broad crown of the erupting permanent central incisor initiates and maintains the resorption of the roots of both the deciduous central and lateral incisors (Figure 1.4). The permanent canine frequently erupts partly mesially, and occasionally at the site of the lateral incisor, while the deciduous canines remain in situ.138
- If the mandibular central incisors are absent, the predecessors persist and may be functional for a long time.
- When the mandibular premolars are missing, the deciduous second molars are usually retained (Figure 1.5)488 as root resorption is not initiated. In the maxilla, the deciduous second molar may exfoliate (due to resorption influenced by the first molar), but not as a rule.
A retained deciduous molar may function for many years, but undergoes wear and physiological changes, such as a reduction in the size of the pulp chamber and hypercementosis (Chapter 8).506 Excessive wear or caries may lead to extraction. Another complication is infra-occlusion (Chapter 4), in which the occlusal surface of the retained tooth stays below the level of the occlusal plane, as the adjacent teeth continue to erupt. In 19–20-year-olds, more than half of the retained deciduous second molars showed 0.5–4.5 mm infra-occlusion.53 The mesio-distal width of the retained tooth exceeds that of the missing mandibular second premolar, which causes a slight malocclusion.53 After late extraction, there is tilting and migration of the neighbouring teeth and overeruption of the antagonist tooth, but this is minimal if the occlusion was stable to begin with.
An early diagnosis of premolar agenesis may be incorrect because these teeth may have delayed development. 12 117 393 648 In 6-year-olds, it is possible not to detect any trace of second mandibular premolar development120 because initiation of calcification of mandibular second premolars may not start before the age of 9 years.127
Agenesis of wisdom teeth is often welcome, because a lack of space within the jaws may inhibit their eruption, causing secondary pathology (Chapter 4). A normal molar relationship (Class I) is observed in these cases.151 Permanent teeth may erupt prematurely when the deciduous predecessors are agenetic.464 Isolated dental agenesis may lead to malocclusion, but dentofacial deviations are mostly minor.656 The alveolar process may be underdeveloped locally. In one study, patients lacking four or more teeth were found to have a smaller cranial base, a shorter maxillary length, a slightly prognathic mandible with anticlockwise rotation, and retroclination of the maxillary incisors.172
Prevention and Treatment
Isolated agenesis in the deciduous dentition does not require treatment, but it is prudent to consider taking radiographs of the patient and their siblings, for counselling and timely treatment of agenetic permanent teeth.
Deciduous molars without successors must be extracted214 at a young age,395 taking into account the relationships between the maxillary and mandibular teeth. Early extraction allows the permanent first molar to move mesially spontaneously without excessive tilting, filling most of the extraction site. Spontaneous space closure occurs if the deciduous mandibular molar is extracted before the root of the mandibular first molar is completed and before the second molar erupts.359 Deciduous second molar extraction at 10–13 years in dentitions with a normal occlusion was found to result in a diastema, which half closed within 1 year by the tilting and migration of the adjacent premolars and canines, and, in particular, mesial tilting of the first mandibular molars. The closure was enhanced by the displacement of the maxillary first molar due to growth in a downward direction.375 431 Two years later, 10% of maxillary and 20% of mandibular diastemata remained. In contrast with the mandible, a maxillary unilateral extraction did not result in a shift of midline.375 The local width of the maxillary and mandibular alveolar arches decreases considerably after extraction.431
An unstable situation requires orthodontic closure of a diastema. Care must be taken that the anterior teeth do not tip lingually.631 If the contralateral premolar is present, its extraction must be considered. An alternative approach is space maintenance, followed by the placement of an implant or a bridge. Long-term implant survival is around 90%, independent of its location.167 Timing of implant placement depends on vertical alveolar growth, which continues beyond puberty: an implant-supported prosthesis inserted in adolescence will eventually become infra-occluded. Sometimes it is possible to transplant a tooth (Chapter 7) that must be extracted for orthodontic reasons into the site of an agenetic tooth.340
Extraction of retained deciduous molars in adulthood necessitates insertion of implants or bridges for function and aesthetics. However, deciduous second molars that are lacking successors and are retained into adulthood remain functional for a long time.545 In one study, only a few retained second deciduous mandibular molars were lost because of caries or periodontal breakdown at the age of 48 years;545 in a minority of cases root resorption of the deciduous molar will be a problem.364 666
- A patient with agenesis of the permanent maxillary lateral incisors requires orthodontic space closure. In contrast with replacement with partial dentures, moving the permanent canines into contact with the central incisors (Figures 1.6 and 1.7) resulted in a healthier periodontium 7–10 years later424 and greater patient satisfaction.482 Restorative reshaping of such canines with composite creates a cosmetically acceptable emergent incisor profile on the canine.490 If not treated orthodontically, a rather wide diastema will remain. Space maintenance is required to close the diastema with an adequate implant546 or bridge after cessation of the (rapid) alveolar growth. The use of osseointegrated implants in children is problematic for reasons of jaw growth, but is presently under consideration.643
- When the permanent central mandibular incisors are absent, extraction of the predecessors is not indicated. An acceptable prosthetic solution after natural loss of the long-persisting deciduous teeth will require maintenance of the diastema.180
Figure 1.6 Patient with missing maxillary lateral incisors.

Figure 1.7 The canines of the patient in Figure 1.6 have been moved orthodontically into the locations of the agenetic maxillary lateral incisors. The morphology of the canines may be improved by grinding the cusps and building the lateral margins with composite so that the teeth resemble lateral incisors. Note the presence of only three lower incisors.

1.2.2 Oligodontia
The term oligodontia has been defined by various authors as the absence of either four or six and more or eight and more teeth, excluding agenesis of third molars.263 468 648 664 Oligodontia has diverse presentations. Some patients lack many posterior teeth and others lack anterior teeth.468 The pattern of missing teeth is often bilaterally symmetrical. The frequency of oligodontia is low: about 0.1–0.5% people have seven to eight missing teeth.1 47 219 371 485 541 594 664
Oligodontia occurs either sporadically in just one individual26 559 or it may be inherited without other anomalies.583 It commonly occurs in association with Down’s syndrome (trisomy 21116) and syndromes in which the epithelium or its derivatives are involved, such as ectodermal dysplasia with abnormal hair, nails and sweat glands (Chapter 11). When a larger number of teeth are missing or more “stable” elements, especially the maxillary central incisors,468 are absent, the presence of a syndrome should be suspected. Conversely, three or more (inherited) skin conditions require investigating for dental agenesis,517 518 but absence of “stable” teeth is not inevitably a sign of a general disorder.572
In cherubism, a hereditary (autosomal recessive?) painless disorder with oligodontia, the middle and lower part of the face become progressively more and more rounded.335 The cherubic appearance may be enhanced by skin stretching and downward pulling of the lower eyelids, causing an upward directed look.153 467 616
In microsomia I, agenesis and delayed maturation of teeth is related to the severity of the disorder. It affects the face unilaterally, with underdevelopment of the mandibular ramus and adjacent soft tissues, possibly caused by a vascular lesion of the first and second branchial arches.113 175
Hall (1983) mentions 34 syndromes and a number of clefts with isolated dental agenesis or oligodontia,235 but the number is at least 120.660
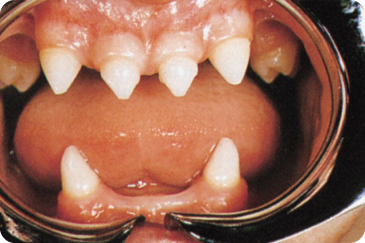
In one study, some 60% of oligodontia patients had ectodermal dysplasia; the other 40% had intermediate severity eczema and asthma, and some experienced hyposalivation.423 “Isolated” oligodontia patients had fewer sweat glands than controls.218 Oligodontia (Figure 1.8) is, moreover, characterised by reduced tooth size423 and morphology (conical crowns, short roots), 11 317 and underdevelopment of the alveolar processes.80 222 317 480 The face tends to resemble that of an edentulous person, with protrusion of the mandible and pouting lower lip, and often a decrease in vertical dimension.
Figure 1.8 Oligodont dentition with hypoplastic and conical teeth.
(Courtesy of Department of Oral Surgery, University of Groningen.)
Heredity
Analysis of family trees suggests an autosomal dominant inheritance pattern in more than half of oligodontia patients.187 213 517 572 Different mutations of the PAX9 gene encoding the PAX9 protein appear to be associated with specific oligodontia patterns, but other genes are most probably involved in specific combinations of multiple missing teeth. PAX9 is expressed in the neural-crest-derived mesenchyme of the mandibular and maxillary arches. MSX1 has been found to be associated with agenetic second premolars and third molars, but PAX9, on chromosome 14,186 was associated with missing first and second molars.327 A mutation in MSX1 was found to be unlikely in family members who, to various degrees, had missing first, second and third molars, premolars and mandibular incisors.213
A PAX9 nonsense mutation changes a chain-termination codon from one that specifies an amino acid into one that does not,633 which results in incomplete protein synthesis and oligodontia.417 A de novo deletion of the proximal long arm at chromosome 14 resulted in developmental defects, but oligodontia was not mentioned in the report.522 A deletion involving the PAX9 locus was observed in a proband with absence of most deciduous and permanent teeth. A frame-shift mutation in PAX9126 encodes an abnormal protein or disrupts the synthesis of the protein completely.633 Identical twins have been found to have a frame-shift mutation and a premature stop codon.125 A missense mutation in the PAX9 gene was found in a family with a distinct oligodontia type.342 The mutation changes a codon specific for one amino acid into a codon />
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


