PATIENT COMPLIANCE IN ORTHODONTICS
Some degree of patient compliance is required for the success of any course of orthodontic treatment. Unfortunately, patient cooperation has diminished in all aspects of health care, and orthodontics is no exception.
Malocclusions featuring skeletal discrepancies (Class II and III) are most affected by lapses of cooperation because patients have been traditionally required to comply by wearing removable appliances, intermaxillary elastics, and extraoral traction in attempts to attain a Class I dental and skeletal relationship. Patient education and motivational techniques are at best temporarily successful in eliciting compliance with these traditional orthodontic biomechanics. The orthodontic specialist now apparently needs charisma and interpersonal skills in addition to tooth-regulation acumen.
Behrents suggests that compliance is the “most important factor in determining treatment success.” Again, unfortunately, patient compliance has decreased. Identifying patients who will be cooperative and then measuring their level of compliance is about as successful as picking lottery numbers. It is also disconcerting that the dose-effect relationships between appliance wear and outcome are poorly correlated in orthodontics. As a result, “noncompliant patient therapies” have become a popular topic in orthodontic continuing education, the literature, and the marketplace.
DEVELOPING A TREATMENT PHILOSOPHY
This chapter reviews a method of treatment for Class II malocclusions that requires only a single phase of mechanics and reduces reliance on patient compliance for consistent and predictable case completion. Orthodontists have become preoccupied with improving their treatment efficiency and efficacy; however, treatment quality, stability, and patient comfort should not be compromised in this pursuit.
On-Time Finishing
Treatment mechanics less dependent on compliance may reduce “cases beyond estimates.” The benefits of improving “on-time completion” percentages in clinical practice include limiting practice overhead and increasing goodwill with both parents and referrers. Reducing extended treatment times also limits “exposure time” for iatrogenic effects, potentially decreasing rates of root resorption, enamel decalcification scars, periodontal concerns, and the incidence of temporomandibular disorder (TMD) symptoms. Orthodontists may then focus attention on other patient compliance issues, such as oral hygiene, reducing scar formation, appliance breakage, and missed appointments.
Moreover, noncompliance therapy is not only for patients identified as “noncompliant”; many patients might benefit from improved efficiency of traditional techniques. Selecting methods for timely and consistent case completion is a logical goal for all patients, especially when the identification of a noncompliant patient seems unpredictable before the patient’s involvement in actual treatment.
One-Phase versus Two-Phase Treatment
Class II malocclusion has been described as “one of the most frequent treatment problems in orthodontic practice,” with a frequency of 37% in preadolescent patients. The development of Class II appears to be promoted and maintained by both facial growth and dental eruption. A deficient mandible has been described as the most common reason, with less than 30% of Class II patients in a group of 8- to 10-year-old children displaying protrusive maxillae. Although a sample of older patients might demonstrate fewer mandibular retrusions, factoring the effects of continued facial growth, the actual percentages might be considered academic, unless you elect to treat later.
It would then seem reasonable to expect that treatments designed to promote mandibular growth (e.g., functional appliances) rather than to restrict maxillary development (e.g., headgear) would be preferred. Consequently, functional jaw orthopedics (FJO) developed as the “growth industry of the 1980s,” with the prevalence of two-phase treatment increasing to approximately 25% of all patients, or one third of all children entering orthodontic treatment at its height of popularity. The strong belief in FJO stimulated the resurrection and creation of many orthodontic appliances, most of which were removable and required excellent patient compliance.
Unfortunately, two-stage treatments, designed to stimulate extra mandibular growth (i.e., functional appliances or arch development “bimaxillary expansion” devices), have little support in the literature. The concerns with most two-phase systems include protracted treatment with long transition periods (often requiring additional appliances or “phase-one orthotics” to prevent immediate relapse), reduced stability, increased iatrogenic effects, and increased financial burden. Therefore a cost/benefit analysis is warranted: do the benefits of early intervention justify the costs of two-phase treatment?
Gianelly argued that “at least 90% of all growing patients can be successfully treated in only one phase by starting treatment in the late mixed dentition stage of development; identified by the exfoliation of all deciduous teeth except the second primary molars.” In 1947, Hays Nance shared a similar philosophy: “Active treatment in the mixed dentition period is desirable only in Class III cases, cross-bites, and Class II cases wherein facial appearance is markedly affected.” Unless we suspend disbelief, there are few, if any, long-term benefits specific to much of what passes for early treatment today. Accordingly, treatment plans featuring a single phase of treatment may be preferable for the majority of patients presenting to an orthodontist’s practice.
DEVELOPING A TREATMENT PHILOSOPHY
This chapter reviews a method of treatment for Class II malocclusions that requires only a single phase of mechanics and reduces reliance on patient compliance for consistent and predictable case completion. Orthodontists have become preoccupied with improving their treatment efficiency and efficacy; however, treatment quality, stability, and patient comfort should not be compromised in this pursuit.
On-Time Finishing
Treatment mechanics less dependent on compliance may reduce “cases beyond estimates.” The benefits of improving “on-time completion” percentages in clinical practice include limiting practice overhead and increasing goodwill with both parents and referrers. Reducing extended treatment times also limits “exposure time” for iatrogenic effects, potentially decreasing rates of root resorption, enamel decalcification scars, periodontal concerns, and the incidence of temporomandibular disorder (TMD) symptoms. Orthodontists may then focus attention on other patient compliance issues, such as oral hygiene, reducing scar formation, appliance breakage, and missed appointments.
Moreover, noncompliance therapy is not only for patients identified as “noncompliant”; many patients might benefit from improved efficiency of traditional techniques. Selecting methods for timely and consistent case completion is a logical goal for all patients, especially when the identification of a noncompliant patient seems unpredictable before the patient’s involvement in actual treatment.
One-Phase versus Two-Phase Treatment
Class II malocclusion has been described as “one of the most frequent treatment problems in orthodontic practice,” with a frequency of 37% in preadolescent patients. The development of Class II appears to be promoted and maintained by both facial growth and dental eruption. A deficient mandible has been described as the most common reason, with less than 30% of Class II patients in a group of 8- to 10-year-old children displaying protrusive maxillae. Although a sample of older patients might demonstrate fewer mandibular retrusions, factoring the effects of continued facial growth, the actual percentages might be considered academic, unless you elect to treat later.
It would then seem reasonable to expect that treatments designed to promote mandibular growth (e.g., functional appliances) rather than to restrict maxillary development (e.g., headgear) would be preferred. Consequently, functional jaw orthopedics (FJO) developed as the “growth industry of the 1980s,” with the prevalence of two-phase treatment increasing to approximately 25% of all patients, or one third of all children entering orthodontic treatment at its height of popularity. The strong belief in FJO stimulated the resurrection and creation of many orthodontic appliances, most of which were removable and required excellent patient compliance.
Unfortunately, two-stage treatments, designed to stimulate extra mandibular growth (i.e., functional appliances or arch development “bimaxillary expansion” devices), have little support in the literature. The concerns with most two-phase systems include protracted treatment with long transition periods (often requiring additional appliances or “phase-one orthotics” to prevent immediate relapse), reduced stability, increased iatrogenic effects, and increased financial burden. Therefore a cost/benefit analysis is warranted: do the benefits of early intervention justify the costs of two-phase treatment?
Gianelly argued that “at least 90% of all growing patients can be successfully treated in only one phase by starting treatment in the late mixed dentition stage of development; identified by the exfoliation of all deciduous teeth except the second primary molars.” In 1947, Hays Nance shared a similar philosophy: “Active treatment in the mixed dentition period is desirable only in Class III cases, cross-bites, and Class II cases wherein facial appearance is markedly affected.” Unless we suspend disbelief, there are few, if any, long-term benefits specific to much of what passes for early treatment today. Accordingly, treatment plans featuring a single phase of treatment may be preferable for the majority of patients presenting to an orthodontist’s practice.
CLASS II CORRECTION
Contributions from both orthopedic and orthodontic factors are common to the resolution of Class II malocclusions. Some treatment effects involve movement of the dentition, and others involve changes in bone (sutural adjustment and growth). To the consternation of FJO enthusiasts, traditional edgewise treatments (often involving extraoral traction and intermaxillary elastics) have demonstrated orthopedic effects that are much the same as those achieved by functional appliances.
Some may be surprised that successful and dramatic orthodontic results were produced before the current preponderance of two-phase treatments that often feature routine “bimaxillary expansion” with jackscrew devices and removable “jaw-growing” appliances. These “modern” mechanics may be more a function of wishful thinking than necessity.
For at least 75% of Class II cases, two-phase functional/edgewise treatment yields results indistinguishable, in terms of facial, skeletal, and occlusal factors, from shorter and more efficiently applied one-phase edgewise therapy. Therefore, the majority of two-stage treatments demonstrate no superior benefits compared with traditional treatment, especially for patients with less than 7 to 11 mm of overjet. This suggests that the selection of two-phase functional treatment may well be a practice management decision rather than one based on biology.
Choosing a Class II Treatment Modality
Indeed, if the final results from the various methods of Class II correction used in the past millennium of orthodontics were “created equal,” it would be wiser to consider the potential effects of limited patient cooperation when selecting an appropriate appliance. Patients only have a limited quantity of “compliance,” and it may not be expressed during preadolescence (perhaps compromising prolonged dual-stage strategies and their inherently protracted two phases of retention).
Because selection of a cooperative patient cannot be guaranteed, it is important to ask if the treatment method chosen is simple, comfortable, and easy to comply with (i.e., the “Keep-It-Simple-Stupid” [KISS] principle). It may be beneficial to bring patients into the decision process and have them help select their own appliance. “If correction by the various mechanisms is virtually the same, what would you choose to ‘wear’ (Fränkel, Bionator, Bio-bloc, twin block, Herbst, jackscrew expanders, headgear), and would you prefer one or two phases of treatment?”
Some might opine that “you cannot develop a practice philosophy based on the scientific literature.” In the current environment, however, featuring evidence-based approaches, the author would argue that it is necessary to reference the literature when selecting treatment modalities designed to be the most effective, efficient, predictable, and comfortable for our patients.
CONTEMPORARY MOLAR DISTALIZATION
One type of Class II correction involves placing “mesially positioned” and rotated Class II maxillary molars into a Class I position. Devices to “distalize” maxillary molars have been developed and include compressed bulbous loops, jigs, springs, magnets, transpalatal arches, and headgears. One method was even patented to “develop” a nonexistent “pre-maxillomaxillary suture.”
Although the term distalization is a neologism, it has become a common descriptor for the biomechanics involved in moving maxillary first and second molars distally and into a Class I molar relationship. More recent molar distalization techniques have included the use of repelling magnets, bulbous superelastic wire loops, and proprietary devices such as the Pendulum (including such variations as Pendex, T-Rex, Pendulum K, AOA Orthodontic Appliances, Sturtevant, Wis.), Jones Jig (American Orthodontics, Sheboygan, Wis.) (i.e., Lokar, Ormco Corp., Orange, Calif.), and Distal Jet (AOA Orthodontic Appliances) (i.e., Keles Slider, Great Lakes Orthodontics, New York, N.Y.). Others are merely alternative means for the application of Class II intermaxillary elastic force (i.e., Bimetric Maxillary Distalizing Arch, Ormco Corp. or Carrière Distalizer, Clínica Carrière, Barcelona, Spain) and, as such, require absolute patient cooperation and may stress mandibular anchorage.
Most of these “continuous force” appliances are not cooperation dependent, may incorporate a modified Nance holding arch or transpalatal connection for some anchorage support, and can produce molar distalization of 1 to 2 mm per month, thereby converting the Class II malocclusion to a more easily resolvable Class I spacing problem in 5 to 9 months. Because there appears to be no substantial advantage to initiating molar distalization methods before the late mixed dentition, these techniques preclude a two-stage regimen.
Typical contraindications to distalization have been patients who feature one or more of the following: significant crowding, bimaxillary protrusion, obtuse mandibular angle, and open bite.
Comparative Analysis of Molar Distalizers
The Distal Jet design, clinical applications, and instructions for use have been described in detail. The clinical effects of the device have also been rigorously documented. Boxes 11-1 and 11-2 outline the advantages of the Distal Jet and evidence-based recommendations.
- •
Esthetic
- •
Simple insertion and activation
- •
Intraoral conversion to a modified Nance holding arch
- •
One appliance serves two purposes: distalizer and holding arch
- •
Less molar tipping
- •
Favorable premolar distal tipping
- •
Minimal vertical effects
- •
No bite plane or jackscrew required
- •
No compliance required
- •
Self-limiting
- 1.
Average starting age: 12 to 13 years.
- 2.
Second molar eruption: slight advantage.
- 3.
Use 240-g nickel-titanium open-coil springs.
- 4.
Construct appliance from first premolars, and permit second premolars to drift distal due to effect of transseptal periodontal fibers.
- 5.
Bend “double-back” wire, inserted in the lingual sheath to rotate molars distally around the palatal root.
- 6.
Check parallelism of construction to occlusal plane and buccal dentition to produce or reduce expansion and bite opening.
- 7.
Level and align only the mandibular dentition with brackets during maxillary molar distalization.
Molar distalization and tipping
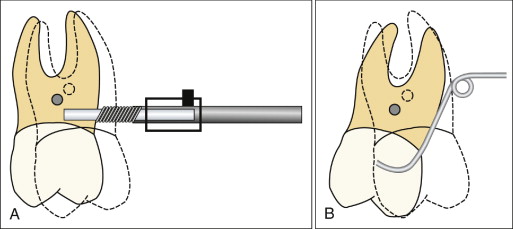
During the typical 5 to 7 months of molar distalization, the Distal Jet has been demonstrated to produce an average of 3.2 mm of distal movement of the maxillary first molar crown. The corresponding amount of distal tip to the molar crown appears to range from 3 to 7 degrees. The magnitude of tipping, however, is often less than with other popular distalizing devices (e.g., Pendulum: 8-16 degrees; Jones Jig: 7-8; GMD: 7; Wilson modular technique: 8; cervical headgear/sagittal appliance: 13; repelling magnets: 7 degrees). The reason is that the Distal Jet forces are applied more apically, through a couple (bayonet wire), closer to the center of resistance of the molars ( Fig. 11-1 ).
Anchorage loss
As the molars are pushed back, spaces tend to open between the molars and premolars. Some of the space results from the distal movement of the molars, but some is also a result of mesial anchorage loss caused by the reciprocal forces applied to premolars (teeth included in the construction framework of Distal Jet appliance). The amount of anchorage loss with this appliance typically varied from 15% to 55% (measured at the premolars). In fact, more anchorage loss was noted when the Distal Jet was combined with maxillary preadjusted bracket mechanics ( Fig. 11-2 ).
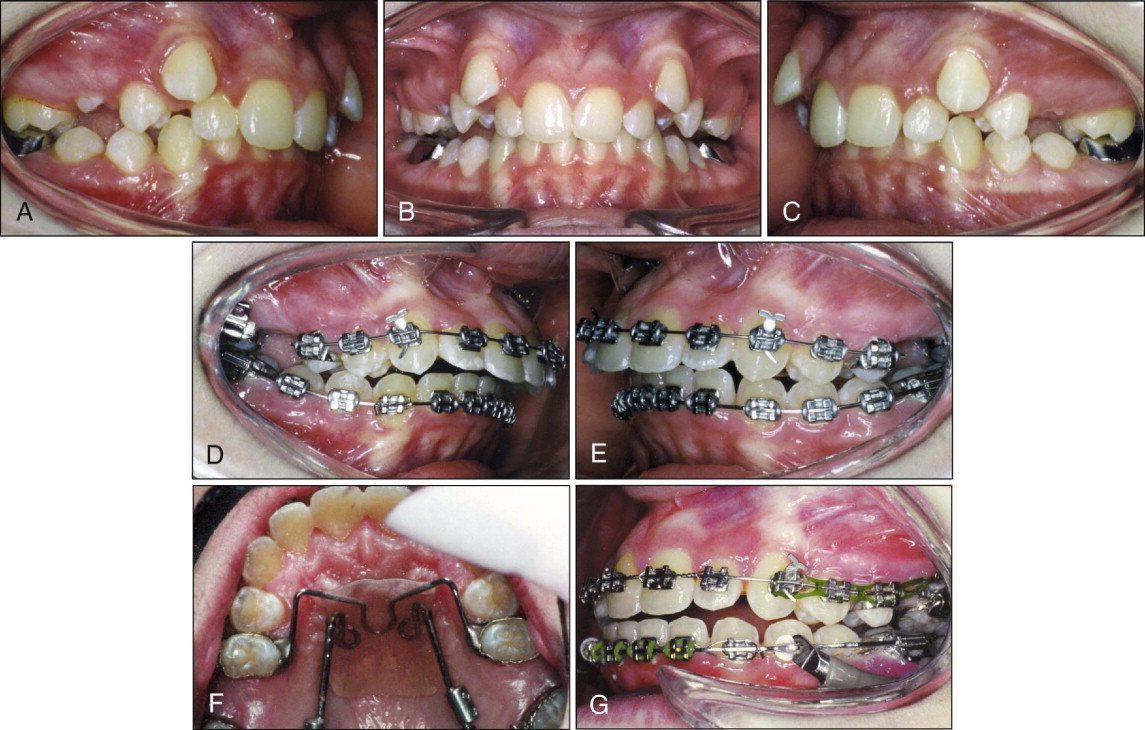

Specifically, an average 10-degree increase in incisal angulation was noted when leveling mechanics, using upper braces (preadjusted appliance), were accomplished concomitant with molar distalization. Despite that a normal incisor angulation was achieved by the conclusion of treatment ( Fig. 11-2, H-M ), there appears to be no advantage to placing maxillary brackets before completing molar distal movement.
Creation of space
The total amount of space created during the Distal Jet molar distalization process ranged widely between 4.6 and 13.4 mm on each side of the dental arch. On average, the space was somewhat less than the amount of space produced by the Pendulum (10-15 mm), although that device yielded substantially more molar tipping.
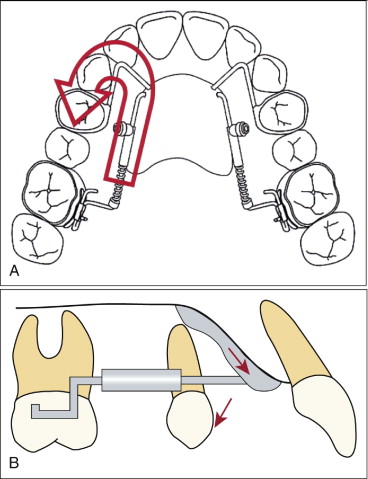
Although maxillary premolars were moved mesially with all distalizers, they curiously tipped distally with the Distal Jet, a finding that was different from other popular appliances. Initially, this effect seemed to make little sense until the biomechanics of the device were examined. Because the forces were applied closer to the center of resistance (via a couple) of the molars and premolars (i.e., more apically), there was more likelihood of mesial bodily movement of the premolars. Forces were applied to the acrylic Nance button in the premaxillary region of the palate such that it had a tendency to migrate occlusally, which caused it to slightly rotate down from the palate ( Fig. 11-3 ). This, in turn, produced the mild, but favorable, distal cant of the premolars, contrasting greatly to the sometimes dramatic mesial flaring of premolars found with other devices (e.g., GMD, Jones Jig, Pendulum). Excessive distal tipping of molars and mesial tipping of premolars, often seen with alternatives to the Distal Jet, are clinically significant for the following reasons:
- •
More molar tipping produces vertical changes (e.g., increases in mandibular plane and lower anterior face height).
- •
More “space” appears to be created (from tipping of molars and premolars), but actually the same amount of usable space (or distalization) is produced.
- •
Subsequent uprighting or paralleling of the tipped molar and premolar roots promotes anchorage loss and is redundant (i.e., a “round-trip”).
When the effects of adverse molar and premolar tipping are accounted for in calculations of the space created during molar distalization, the Distal Jet and the Pendulum appeared equivalent in amount of “usable” distalization. Unfortunately, later uprighting of molars and premolars must be accomplished with the Pendulum, and there was also more potential for adverse vertical effects caused by the molar tipping. Unfortunately, the action of the Pendulum is also not self-limiting, unlike the Distal Jet appliance, and unattended use may produce adverse effects. In contrast, the Distal Jet produced no significant increase in vertical dimension (no molar extrusion, no change in mandibular or occlusal plane angles, no undesirable change in lower anterior face height), even for patients who initially presented with more obtuse mandibular plane angles.
Timing of treatment
Most recommendations for the timing of distalization have been to treat “earlier,” before the eruption of the second molars. In the mixed dentition, less anchorage loss reportedly is produced because there are only the two first permanent molars to push distally.
The opposite response was found for the Distal Jet; namely, that waiting to treat until at least partial eruption of the second molars has occurred is a slight advantage. No greater anchorage loss appeared to occur, and there was less adverse tipping of the first molar, because the center of resistance of the molar was moved occlusally when it was “braced” against the erupting second molar ( Fig. 11-4 ). Graber reported the same effect when using the cervical headgear for distalizing.
If the contribution of greater amounts of molar tipping (when second molars are unerupted) were included in calculations of efficiency in studies examining other distalizing devices, similar conclusions (e.g., starting treatment later) may have been attributed to these devices as well.
Molar rotation and expansion
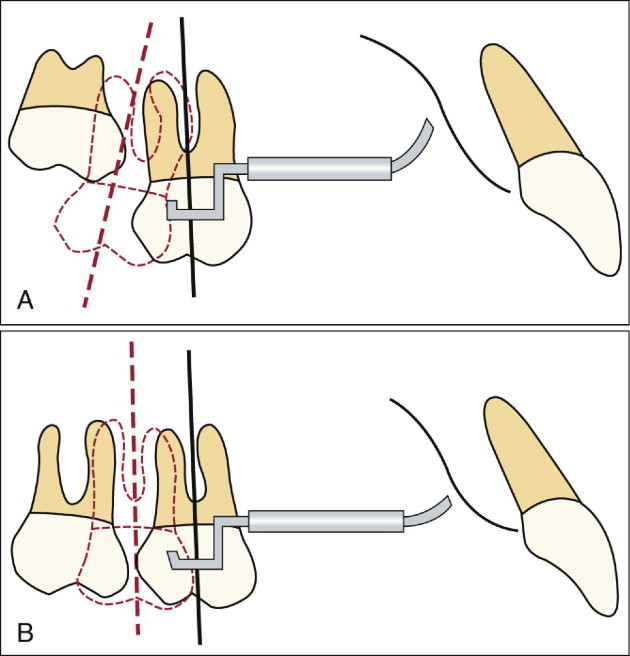
Lemons and Holmes reported that a majority of patients with Class II malocclusions exhibit maxillary first molars that are rotated mesially around the palatal root. In other words, the palatal root may be in a normal, Class I position despite giving the clinical appearance of Class II when the first molar is viewed from the buccal surface. The implication is that, in some cases, simply producing a distal rotation of the molar will produce a Class I molar relationship for many patients.
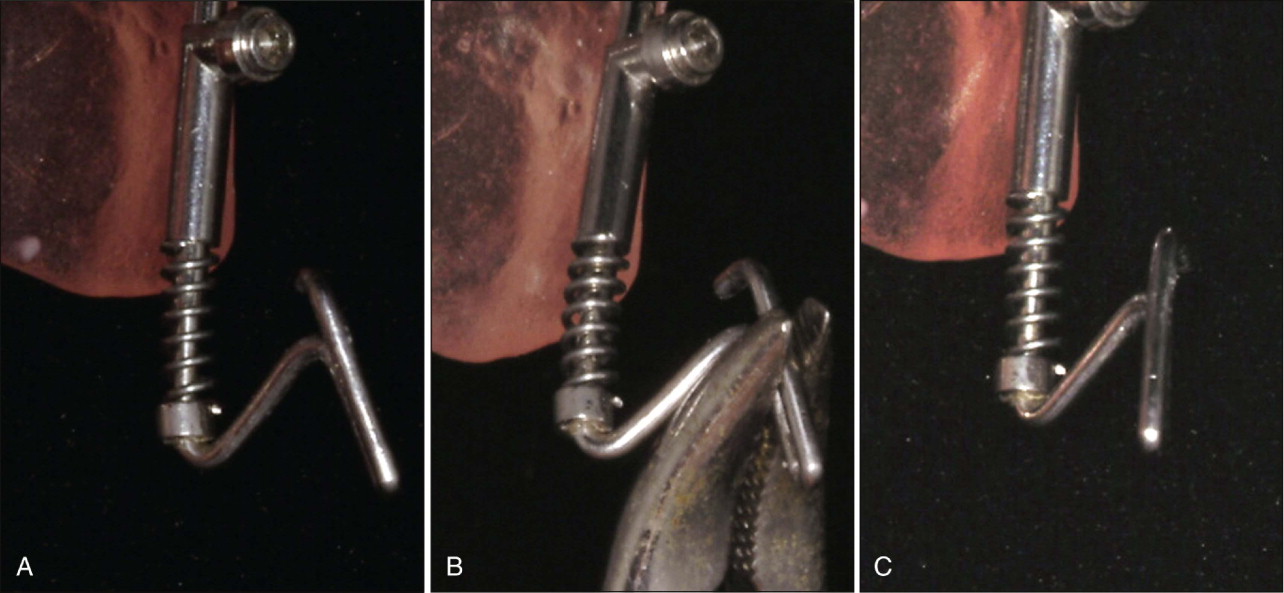
Molar distalizing appliances that produce forces on the lingual surfaces of the upper molars (Distal Jet, Pendulum, GMD) may produce additional inappropriate mesial rotation. A simple preventive solution has been described for the Distal Jet. Before delivering the device, a utility pliers is used to bend the double-back wire (inserted into lingual sheath on maxillary first molar band) to produce a distal molar counterrotation ( Fig. 11-5 ), similar to the bend described by McNamara and Brudon for adjusting transpalatal arches. In this manner, the Distal Jet may produce some corrective molar rotation before or during concurrent molar distalization. Also, most preadjusted appliance prescriptions have some degree of corrective molar rotation built into them as well.
Some degree of maxillary expansion reportedly is required for the correction of Class II malocclusions. Unfortunately, this implies that some type of active palatal expansion is required in the treatment of Class II, when in the absence of posterior crossbite, separating the midpalatal suture is not a prerequisite. Although the Pendulum requires a jackscrew to counteract the adverse constriction of molars that it produces, the Distal Jet yields an average of 3 to 4 mm of expansion (across the molars without a jackscrew) simply because of the divergent nature of its construction ( Fig. 11-6 ).


FIXED FUNCTIONAL APPLIANCES
Orthopedic change, most often attributed only to functional appliances, is an undeniably important factor of Class II correction for the growing patient. Mandibular protraction or advancement is the one feature that is common to all functional appliances. Johnston described this jaw advancement as “taking out an installment loan” against future growth. Holding the mandible forward is the assumption of that loan, while eventual condylar growth and remodeling “pays back” the loan over time. Fixed functional appliances, such as the Herbst (Dentaurum, Ispringen, Germany) or Jasper Jumpers (American Orthodontics, Sheboygan, Wis.), are able to produce mandibular protraction independent of patient compliance.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


