Chapter 33 Zetapalatopharyngoplasty (ZPP)
1 INTRODUCTION
Due to its limited success in curing obstructive sleep apnea/hypopnea syndrome (OSAHS),1 many adjunctive procedures and modifications were proposed after the introduction of the classic uvulopalatopharyngoplasty (UPPP) by Fujita et al. in 1981.2 Its role as part of a comprehensive treatment plan remains, however, solidly accepted in most situations in which the palate, with or without the tonsils, is contributing to airway turbulence and obstruction. The goal of UPPP is to widen the airspace in three areas:
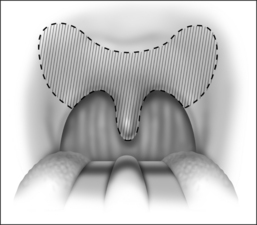
This is accomplished through two components: (a) the palatoplasty component, which involves palatal shortening with closure of mucosal incisions; and (b) the pharyngoplasty component, which is composed of a classic tonsillectomy with pharyngeal closure. These goals, however, are not always achieved with classic UPPP and, in spite of our best efforts, patients may end up with an extremely narrow palatal arch in which the diameter of the oropharyngeal inlet is decreased due to a forward approximation of the posterior palatal mucosa. The resulting new shape of the free edge of the palate is triangular, rather than square. Further contraction of the wound occurs due to scarring secondary to the resection of the posterior tonsillar pillars, and additional narrowing is caused, which further affects long-term results (Fig. 33.1)3 (see also Chapter 32: Submucosal Uvulopalatopharyngoplasty). Additionally, patients who previously underwent tonsillectomy are particularly poor candidates for classic UPPP due to scarring or absence of the posterior pillar from the previous tonsillectomy. These patients have an already narrowed space between the soft palate and the posterior pharyngeal wall and often do not have any redundant pharyngeal folds. Important modifications of the classic UPPP proposed by Fairbanks, in which the posterior pillar is advanced lateral cephalad in order to widen the retropalatal space,4 are, hence, not possible. It is well known that when UPPP fails, the severity of obstruction may actually worsen.5 It became apparent that appropriate selection criteria needed to be implemented in order to identify the patients with a higher likelihood of cure after UPPP. A staging system introduced by Friedman et al.6 identified that patients with anatomic stage I disease (Friedman Tongue Position (FTP) I and II) with large tonsils have a better than 80% chance of success, whereas patients with stage II and III disease (FTP III and IV) are less than ideal candidates and should therefore undergo a combined procedure that addresses both the palate and the hypopharynx. The zetapalatopharyngoplasty (ZPP) technique was developed as a more aggressive technique for patients with stage II and III disease. This includes all patients who have had previous tonsillectomy, as well as patients with small tonsils and those with unfavorable tongue positions. A modification, useful for revision UPPP, is presented in Chapter 62.
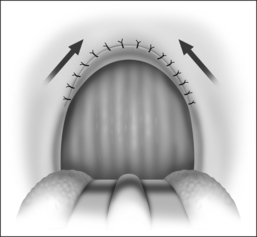
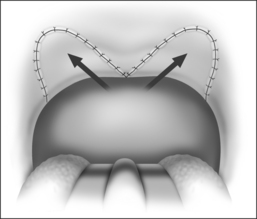
The goal of ZPP is to widen the space between the palate and the posterior pharyngeal wall, between the palate and the tongue base and to either maintain or even widen the lateral dimensions of the pharynx. This is accomplished by changing the scar contracture tension line to an anterolateral vector and by widening the anteroposterior and lateral oropharyngeal air spaces at the level of the palate. By splitting the soft palate and retracting it anterolaterally, an effective anterolateral pull is created, which actually continues to widen the airway as healing and contracture occur (Fig. 33.2). None of the palatal musculature is resected, in spite of the aggressive palatal shortening, thereby addressing and minimizing the risk for permanent velopharyngeal insufficiency (VPI). This procedure is performed with adjunctive tongue base reduction by radiofrequency (TBRF), which addresses the hypopharyngeal airway.
2 PATIENT SELECTION
Specific criteria for ZPP include patients classified as stage II and III according to Friedman’s Anatomic Staging System7 (see also Chapter 16). Because ZPP produces a significant widening of the retropalatal space, it is an aggressive procedure, with significant temporary VPI and the risk for permanent VPI. It should be reserved for patients with moderate to severe OSAHS with moderate to severe symptoms. It is not a surgical option for snoring only.
3 SURGICAL TECHNIQUE
The surgical technique for the modified ZPP is illustrated in Figures 33.3 to 33.10.
< div class='tao-gold-member'>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


