Veneers—From Planning to Recall
The term “Hollywood smile” was coined by Dr. Charles Pincus during the 1930s. At the 1937 meeting of the California State Dental Association he said: “The average dentist always considers articulation and function, while only very few consider aesthetics. We should not forget, however, that we are dealing with an organ that characterizes and can change an individual’s entire personality. A beaming smile, a straight row of natural white teeth is an important component of a characteristic of a personality that is very difficult to understand.” To help movie stars to get a beaming white smile, Dr. Pincus invented the veneer technique—wafer-thin ceramic shells that were glued onto teeth. It was a very expensive method that was affordable to only a few. The technique was not further developed until new bonding methods became available, and it has been successfully used since 1985 (Calamia 1985).
The Advantages of Veneers
Veneers are labial partial crowns. Their advantages compared to crowns are so major that they should be preferred to crowns in almost all cases.
Color and Aesthetics
It is only occasionally possible to achieve a similarly perfect aesthetic result with crowns as with veneers. Color, form, surface, individual characterization through internal and external staining, color corrections during cementation with special cement colors, and the contact lens effect, which makes these restorations invisible—all these factors lead to a perfect restoration.
Durability and Tooth Conservation
Ceramic veneers have high abrasion and color stability. With the new bonding methods, the risk of fracturing veneers is presumably smaller than that of metal or all-ceramic crowns.
Only little tooth substance is removed (0.5–0.75 mm) during veneer preparation.
Function
Since the veneer itself is in most cases limited to the labial surface and the incisal part of the clinical crown, postoperative functional complications can also be avoided. Particularly in patients with deep bites there is rarely sufficient space on the lingual side for conventional crown preparations. Also, lower front teeth can only in rare cases be treated with traditional crown techniques and be aesthetic, retain functionality, and simultaneously protect the pulp. Veneers are, therefore, far superior to crowns.
Strength
The new generation of dentin adhesives and cementation materials makes it possible to extend the list of indications for veneers. It is no longer necessary that all cut margins are in the enamel. The strength of the bond of etched and silanized porcelain, adhesively bonded with the new bonding materials to enamel and dentin, has opened a new era. The bond strength values of etched porcelain bonded with composite cement are as high as systems consisting of composites bonded to etched enamel.

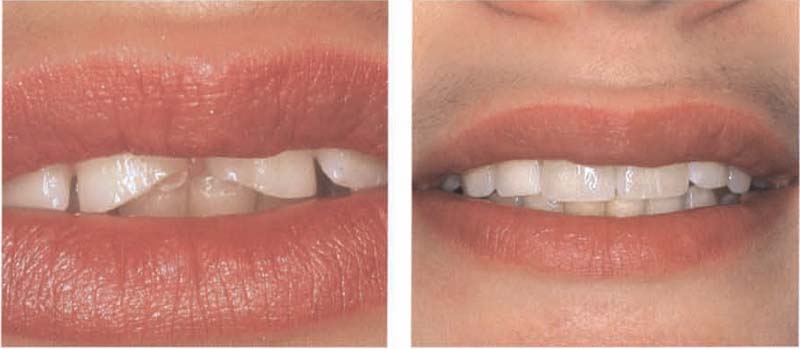
407 Shortened upper incisors
Acid erosion, toothbrush abrasion, and bruxism have led to a significant loss in coronal length of this patient’s upper front teeth.

408 Reconstruction using veneers
Aesthetics and function of the upper incisors were restored with veneers.
Dental technician: R. Schubert
Furthermore, the coefficient of thermal expansion of the veneers is comparable with that of the natural tooth structure. No other restoration is as stable and durable. This is astonishing, because in the unbonded condition the veneer is very fragile. However, as soon as it is adhesively bonded to the tooth, it develops an extremely high tensile and flexural strength.
Periodontium
It is not necessary to hide the veneer margin under the gingiva as is the case with front crown margins. Since they are invisible, the margins are supragingivally or slighly subgingivally placed and sealed with insoluble composite cement, resulting in gingival health conditions that are usually better than with crowns. However, finishing the veneer margin is a very difficult and demanding task.
The Disadvantages of Veneers
Irreversibility
Tooth substance must be removed. The restorations can not be tried-in and be cemented temporarily. If the veneer is put in and attached, it is not possible to correct it later. However, a veneer can be removed (this is only possible through grinding) and replace it with a new veneer or crown.
Cost
Placing a veneer is a very demanding dental activity. For the ceramist in the laboratory, it is also a big challenge again and again to accommodate color, form, surface structure and individual characteristics on small areas. All this leads to relatively high costs.
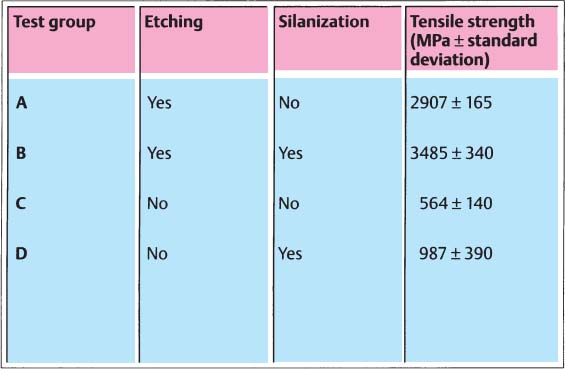
409 Effect of conditioning used on the ceramic surface on the tensile strength of the restoration
The surfaces of all-ceramic restorations should be conditioned before cementing: etch with hydrofluoric acid and silanate (exception: In-Ceram). The combined treatment (group B) increases the tensile strength when compared to the untreated control surfaces (group C) by a factor of approx. 6.
(Adapted from Hsu et al. 1989)
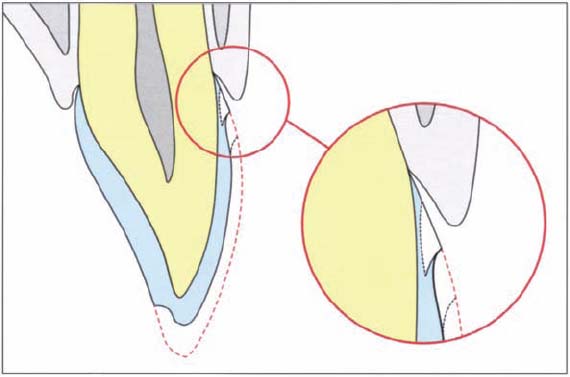
410 Cervical margin
The margins of veneers do not need to be hidden below the gingival margin as is the case with crown margins. They can end at the gingival margin or finish slightly supragingivally. The veneer margins are not visible in the mouth because of the contact lens effect: like a contact lens, the edges of a veneer cannot be recognized in the moist environment of the oral cavity.
Indications and Contraindications
Special indications:
— Tooth fractures in teenagers.
— Single and strongly discolored nonvital teeth.
— Large labial erosions and front teeth with extensive cervical restorations.
— Strong discolorations that cannot be removed by bleaching or through micro abrasion.
— Extensive enamel defects.
— Occlusal and incisal overlays in the anterior and posterior regions caused by acid erosion (bulimia, anorexia nervosa).
— Deep bite with or without contact.
— On lower front teeth instead of crowns.
— Closing a diastema.
— Correcting minor malaligaments.
Contraindications:
— Extreme bruxism
— Front teeth with too extensive composite restorations and with too large destructions
— High caries activity, lack of dental awareness
— Poor oral hygiene
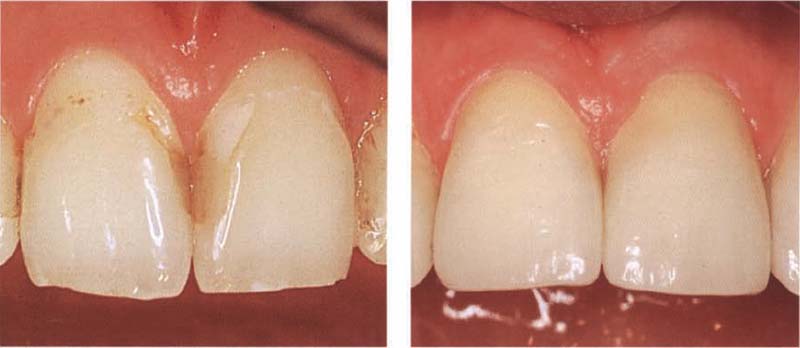
411 Extensive cervical defects
Left: During puberty many teenagers have high caries activity that frequently results in large cervical cavities.
Right: The teeth have been restored very aesthetically with veneers.
Dental technician: A. Schmidseder
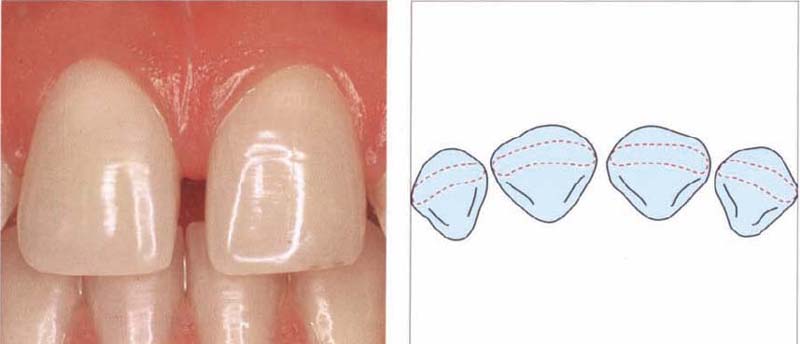
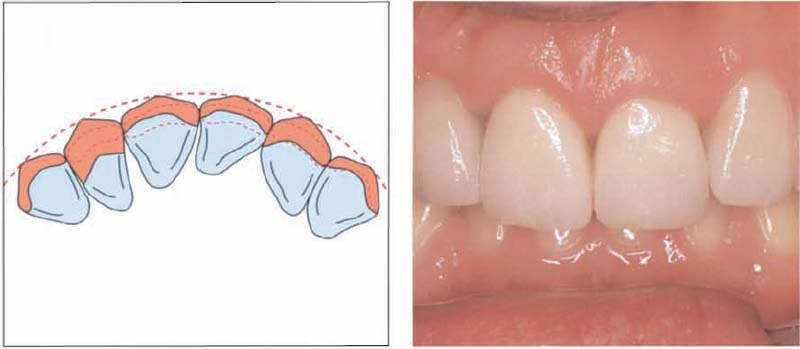
412 Diastema between the upper incisors
A diastema cannot only be closed with direct composites, but also very aesthetically with ceramic veneers.
Left: Situation before treatment.
Right: Graphic representation.
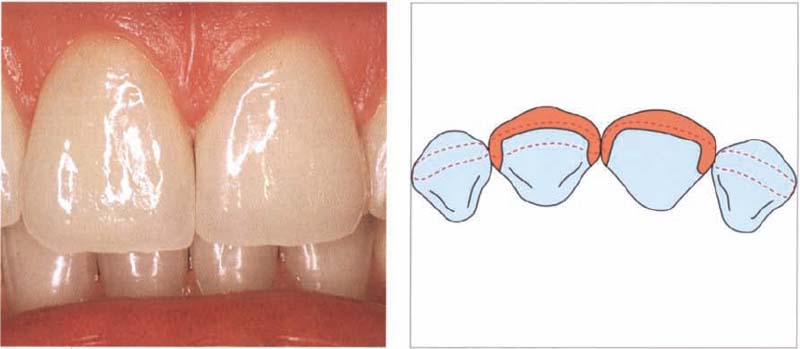
413 Situation after restoration with veneers
Left: Cemented veneers.
Right: The preparations are cut through to the palatal surface so that the proximal spaces can be closed with the ceramic veneers.
Dental technician: R. Schubert
414 Veneers instead of orthodontics
Many adults have already been treated orthodontically and do not wish any further orthodontic treatment. Slightly malpositioned teeth can alternatively be treated with veneers. The resuls are very good.
Left: The labial surfaces of teeth 12, 11, and 22 must be moved forward, while 21 needs to be moved backwards in order to achieve a symmetrical front.
Right: Preoperative situation.
415 After reconstruction
After the wax build-up, it was clear that the teeth could be reconstructed with veneers very well.
Left: Planned correction of repositioned teeth treated with veneers.
Right: Situation after treatment.
Dental technician: R. Schubert
416 Reconstruction of fractured front teeth
It is especially important that crowns should not be used to reconstruct teenagers’ fractured front teeth, as appearance is highly valued in this age group and is important for self-esteem. All-ceramic veneers are an ideal solution.
Left: A 13-year-old girl with fractured incisors.
Right: Veneers have been used to reconstruct the fractured incisors.

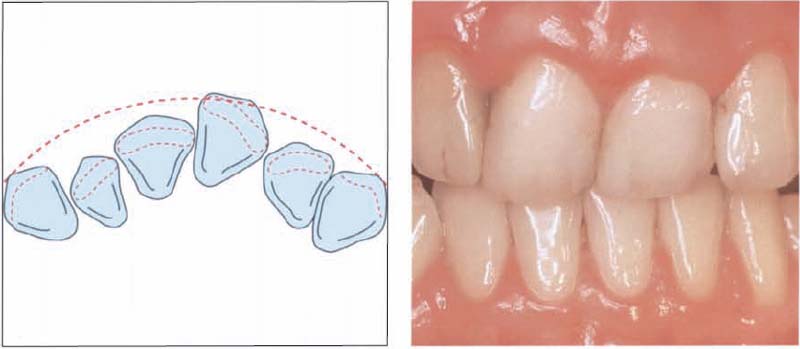
417 Reconstruction of the lower incisors
Defects on lower incisors are not easily reconstructed aesthetically with crowns. All-ceramic veneers withstand high pressure and they are therefore suitable for reconstructing lower front teeth.
Left: Defective and tightly spaced lower incisors.
Right: Reconstruction with veneers.
Dental technician: A. Schmidseder
Diagnostics and Treatment Planning
With any adhesively bonded restorations, a carefully planned and enforced hygiene phase is especially important. Patients must be aware from the beginning that they must come regularly to the recall sessions. The weakness of all bonded restorations is the bond. The adhesive cements are only moderately filled composites that have higher plaque retention and cause a higher risk of secondary caries.
Initial Hygiene Session
1. Investigation of causes for changes to the front teeth. If particular nutritional factors were involved in the discolorations, this should be pointed out to the patient before treatment begins. Acid-containing foods can also change the surface of the ceramic. Also, parafunctions or habits that possibly lead to abrasion of the front teeth should be mentioned and recorded on the patient’s dental chart.
2. Oral hygiene must be adapted to the restorations. Toothpastes with low pH values or high abrasiveness change the ceramic surface over time. Therefore, an individual oral hygiene instruction program is presented and nutrition advice is given before treatment begins.
3. After a thorough professional tooth cleaning, the tooth color and the patient’s desired color are carefully recorded on the chart. Taking intraoral photographs is always recommended. A complete set of radiographs and a panoramic radiograph are also required for the treatment planning.
4. Finally, study models are prepared. If the plan is to change the tooth form/tooth length or to close a diastema, these changes should be planned in a diagnostic wax-up. This facilitates communication with both patient and laboratory.

418 Acid erosions
Rebuilding acid-eroded anterior and posterior teeth is best done with new adhesives. All lingual surfaces of the upper and lower teeth of this 17-year-old patient have been eroded through frequent consumption of acid-containing soft drinks (coke, soda).
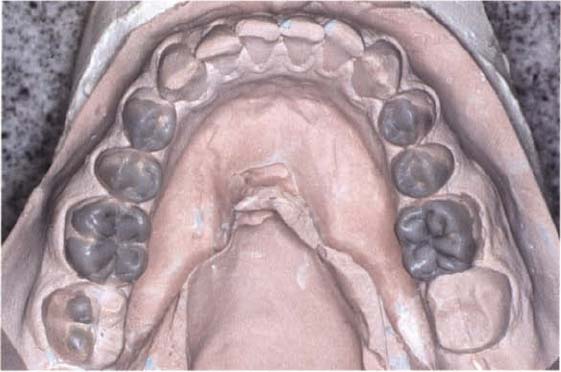
419 Lower jaw model of the same patient rebuilt with wax
Whenever a reconstruction of tooth length, tooth form, or occlusion is planned, a diagnostic wax up of the occlusion should be made.

420 Cemented veneers and partial crowns covering acid erosions
Left: Finished treatment with ceramic partial crowns and veneers.
Right: Occlusal overlays on the model.
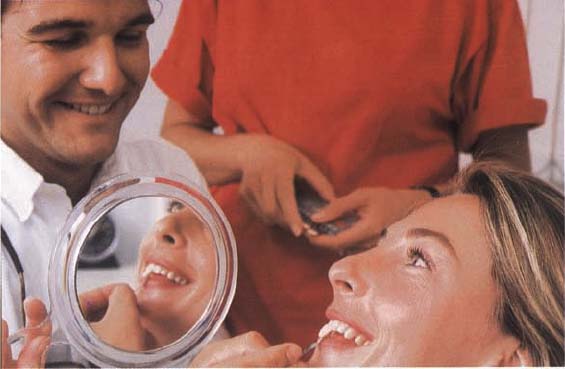
421 Determining the treatment goal
The treatment goal should be decided at the beginning of the treatment: which tooth-color, form, and size?
Patients must participate in choosing the tooth color. Patients themselves must finally determine whether the existing tooth color should be retained or be modified according to their wishes.
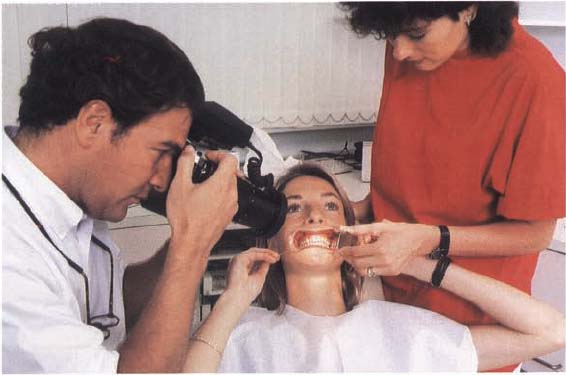
422 Documentation of the initial situation by means of intraoral photograpy
In addition to radiographs, a photo-status is also part of treatment planning.
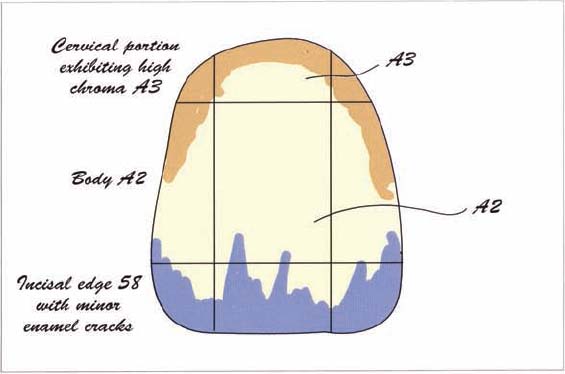
423 Color map of a central incisor
Before beginning preparation, not only existing, but also the desired tooth color should be determined and recorded. In addition, the layering of the remaining teeth should also be recorded. This is best done in the form of a color map that is prepared by the dental technician.
Preparation
In contrast to crown preparation, the preparation of veneers is a very simple dental procedure. If a study model and a diagnostic wax-up are available beforehand, the goal of treatment can be planned and visualized, which accordingly facilitates the preparation design. If the task only involves restoring existing ena/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


