Chapter 29 Uvulopalatopharyngoplasty
1 INTRODUCTION
Although the surgical armamentarium for snoring and obstructive sleep apnea (OSA) has, in the last several years, expanded significantly to include many procedures, uvulopalatopharyngoplasty (UPPP) still remains the most widely performed operation for these conditions. The procedure was first introduced by Fujita in 1981 and is designed to enlarge the airway lumen at the level of the velopharynx and decrease the collapsibility of the pharyngeal walls.
2 PATIENT SELECTION
Physical examination factors important in airway evaluation are:
There are no widely accepted standardized methods or algorithms and frequently surgeons utilize their own judgment in interpreting such indices for patient selection. General points by which UPPP candidates can be identified are seen in Table 29.1. It should be pointed out that when UPPP is performed as part of a multilevel approach, most of these criteria are not relevant.
| Posterior nasal spine to uvula tip distance Tonsil size Posterior airway space Mandibular plane to hyoid distance Friedman tongue position Absence of retrognathia Absence of retroglossia Absence of hypopharyngeal narrowing Absence of lateral pharyngeal wall bulging Absence of morbid obesity Absence of sagittal orientation of airway |
<38 mm +++−+++ >10 mm <27 mm I or II BMI>40 |
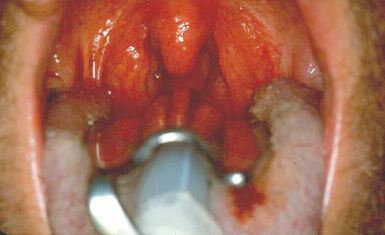
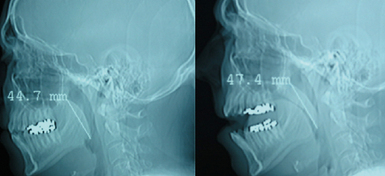
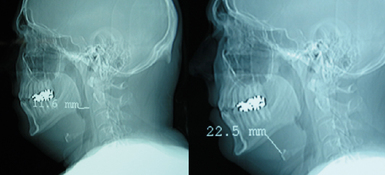
In general patients with large tonsils, elongated uvula and palatal redundancy position who do not have hypopharyngeal narrowing or tongue enlargement and are not extremely obese will be advised to have UPPP (Figs 29.1 and 29.2). Because of its relative simplicity and low morbidity UPPP is usually performed as part of a multilevel approach in many patients, even if there is no overt evidence of velopharyngeal pathology.
3 TECHNIQUE
Step 1
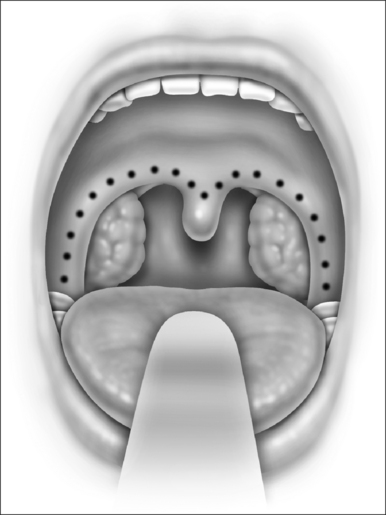
Following orotracheal intubation and deep muscle relaxation, the mouth gag is positioned. This routinely provides adequate visualization and exposure. Local infiltration with epinephrine solution is not performed. In the past the amount of palate to be resected was determined by gently pushing the palate to the posterior pharyngeal wall and marking on its ventral surface the point where the palate met the posterior pharyngeal wall. Currently soft palate resection is conservative and is determined by gently curving the anterior pillar incision towards the base of the uvula, leaving only 5–10 mm of soft palate to be resected. The incision is marked with electrical cautery on the most lateral aspect of the anterior pillar in order to maximally resect this structure and the underlying palatoglossus muscle. The incision is then gently curved towards the base of the uvula and is continued in an identical fashion onto the opposite side (Fig. 29.3).
< div class='tao-gold-member'>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


