Fig. 12.1
Schematic transition between procollagen chains, nucleated under the influence of the C-propeptide. The procollagen trimer is transformed into collagen, a process followed by collagen fibrillation (Linsennnmayer 1981)
12.2 Enamel Surface
Smooth (bands of smooth enamel prisms) or pitted (associated with the end of prisms reaching the enamel surface) surfaces are seen in enamel. They are associated with perikymata, where the crystals are radially oriented. Circadian rhythms and approximately an 8-day periodicity are apparent (Newman and Poole 1974) (Figs. 12.2 and 12.3).
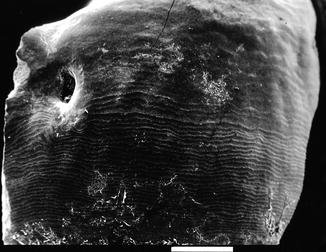
Fig. 12.2
In the cemento-enamel junction, the cementum is overlapping enamel (a). In (b) cement and enamel are continuous, forming an edge-to-edge structure. In (c), gaps are obvious between root cementum and exposed dentin. The 4th missing figure would be related to enamel overlapping dentin, a very seldom case
Fig. 12.3
After cleaning the enamel surface, perikymata are visible. They form alignments
12.3 Morphology of the Cemento-Enamel Junction
At the cemento-enamel junction (CEJ), the following tissue interrelationships were observed:
-
Pattern I: The cementum overlaps the enamel (42–60 %); the cementoblasts produce an afibrillar cementum, dense and laminated, devoid of collagen fibrils with a 64 nm periodicity.
-
Pattern II: Edge-to-edge interrelationship between cementum and enamel (situation seen in 30–41 % of the teeth).
-
Pattern III: There is a gap between root cementum with exposed dentin (10–12 %) (Arambawatta et al. 2009).
The intermediate cementum is a narrow zone of highly calcified tissue. It is located between the most external layer of dentin (granular Tomes’ layer) and the layer of acellular cementum. It is referred to as “the hyaline layer of Hopewell-Smith.” The intermediate cementum layer contains enamel matrix proteins and is a product of Hertwig’s epithelial root sheath. A possible role in wound healing is hypothesized (Harrison and Roda 1995).
The cemento-enamel junction and cementum act as stress damper, decreasing stresses in the periodontal ligament (PDL) and alveolar bone under loading. It influences the stress distribution within the tooth supporting structure.
12.4 Erosive Tooth Wear (Figs. 12.4 and 12.5)
Fig. 12.5
(a) Circumpulpal dentin with open tubuli; (b) sclerotic dentin. Tubules are filled by intratubular mineral precipitations. (c) Globular structures of cement along the root surface
The clinical diagnosis “erosion” is made from characteristic deviations from the original anatomical tooth morphology, thus distinguishing acid-induced tissue loss from other forms of wear (Ganss and Lussi 2014). Tooth wear results from four pathologies: abrasion, due to the interaction between teeth and other materials; attrition, due to tooth-tooth contact; erosion, due to hard tissue dissolution by acidic substances; and abfraction, which intensifies wear by abrasion and/or erosion (Shellis and Addy 2014) (Figs. 12.3 and 12.4). Engineering analyses demonstrate theoretical stress concentration at the cervical areas of the teeth. Abfractions present primarily at the cervical region have typically wedge-shaped, with sharp internal and external angles. They are C-shaped lesions with rounded floors, V-shaped lesions, and Mixed-shaped lesions with flat cervical and semicircular occlusal walls (Levrini et al. 2014). Usually observed on the buccal surface at the cemento-enamel junction, its prevalence varies between 27 and 85 % (Sarode and Sarode 2013). Excessive horizontal tooth brushing can also cause the V-shaped lesion. Occlusal stress produces cervical cracks that predispose the surface to erosion and abrasion. Most data from the literature shed lights on the different possibilities, although still hypothetical. Extrinsic factors (acid vitamin C supplements, acid foods and drinks) and intrinsic factors (gastrointestinal reflux, eating disorders such as bulimia and anorexia) contribute to cause erosion. The lesions were characterized as being unrelated to bacteria. The characteristics of abfractions are the following: in erosion, characteristic pitting is seen on enamel. In abfraction the form of wedge-shaped lesion is clearly located at the cervical level. Dental and non-dental disorders induce specific morphology and mechanisms that differ from acid etching and bonding.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


