The patient was a boy with a Class II skeletal and dental relationship, a large overjet, an impinging overbite, and a steep mandibular plane angle. Treatment started with the Twin-block appliance combined with high-pull headgear to promote growth of the mandible, restrain the maxilla in the anteroposterior and vertical planes, and improve his profile. This was followed by extraction of the maxillary second premolars and the mandibular first premolars. Then fixed appliances were used to align and level the dentition. Pretreatment and posttreatment records are shown, and the treatment results are stable 2 years after debonding.
Functional appliances have been used for many years in the treatment of Class II malocclusions. Alteration of maxillary growth, improvement in mandibular growth and position, and change in dental and muscular relationships are the expected effects of these appliances.
The Twin-block appliance, originally developed by Clark, is a widely used functional appliance for the management of Class II malocclusion. It combines splints with extraoral force and functional orthopedic forces. The appliance can be worn most of the time, with the advantage of allowing nearly a full range of mandibular movement, easy acclimation, and reasonable speech. Its popularity also comes from its high patient acceptability and its ability to produce rapid results.
High-pull headgear is used in Class II patients with increased lower facial height. Teuscher suggested that forward and downward growth of the maxilla could be altered, and that the mandible could also change its growth direction to a more forward and upward position with condylar adaptation using the high-pull headgear.
Functional appliance therapy is followed by comprehensive fixed-appliance therapy with or without extractions. Extraction of 4 premolars is indicated primarily for dental crowding, cephalometric discrepancy, or a combination in growing Class II patients.
This case report demonstrates the use of the Twin-block appliance and high-pull headgear in a skeletal Class II Division 1 patient with a retrognathic mandible, protruding maxillary anterior teeth, excessive overjet, and complete overbite. By means of extraction of the maxillary second premolars and the mandibular first premolars, a well-aligned and leveled dentition and an acceptable profile were achieved.
Diagnosis and etiology
The patient, a Chinese boy aged 12 years 2 months, was in fair health and motivated for treatment with the chief complaint of protruded maxillary anterior teeth and a receding chin for 6 years. He had been biting his lip since eruption of the deciduous dentition. He was introverted and had poor self-esteem, despite his normal medical history. His father had a similar profile of protruded maxillary anterior teeth.
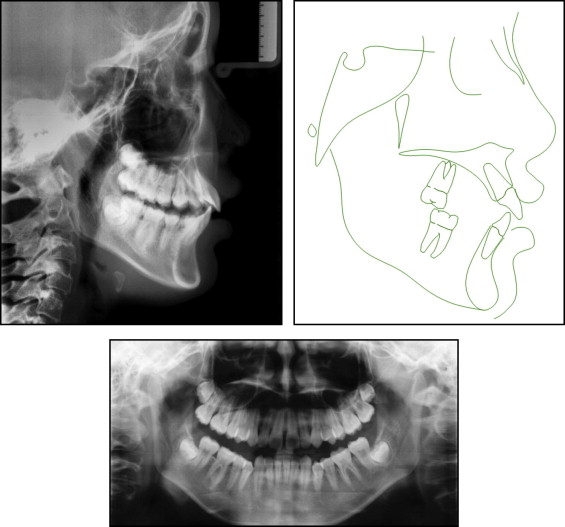
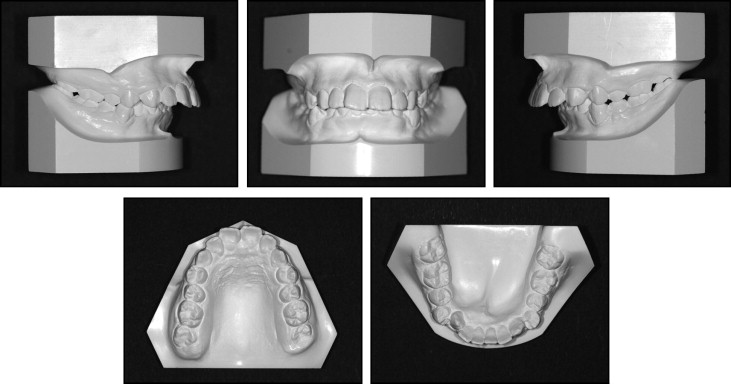
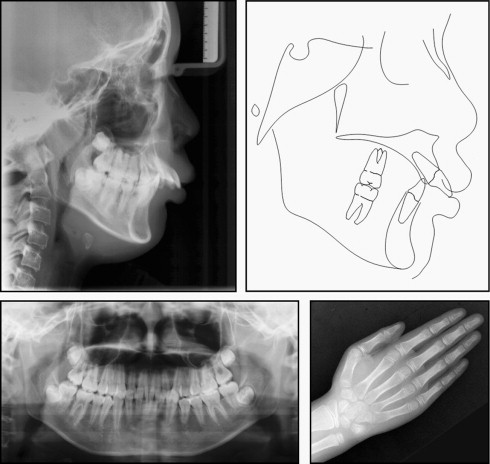
The facial photographs indicated a convex facial appearance, protruded lips, and moderate exposure of the maxillary incisors ( Fig 1 ). He had a normal range of mandibular motion and no joint noise or pain. The midline of the mandible was shifted 2 mm to the right. Other intraoral findings included gingivitis of the incisors, a short lingual frenum, and swollen tonsils. He had a Class II Division 1 malocclusion (bilateral full Class II molars and canines) with a 15-mm overjet and an impinging overbite. Mild maxillary and moderate mandibular crowding as well as mesial inclination of mandibular posterior teeth were observed. The curve of Spee was severe (6 mm), and the Bolton analysis was 78% anteriorly and 88.4% totally. The cephalometric analysis confirmed a skeletal Class II jaw relationship with a retrognathic mandible and a steep mandibular plane angle. Additionally, the maxillary and mandibular incisors were labially inclined. The panoramic radiograph showed tooth buds of 4 third molars and symmetric bilateral joints. A hand-wrist radiograph showed that he was at the stage of a growth spurt ( Figs 2 and 3 ).

The etiology of this patient’s malocclusion was probably a combination of his lip-biting habit and genetic factors.
Treatment objectives
The treatment objectives were to correct the skeletal Class II malocclusion (retrognathic mandible), improve his overjet and overbite, solve the dental crowding, and improve his facial appearance. Cessation of the lip-biting habit was considered essential. Much attention would be given to controlling the vertical growth of his molars because of the steep mandibular plane angle.
Treatment objectives
The treatment objectives were to correct the skeletal Class II malocclusion (retrognathic mandible), improve his overjet and overbite, solve the dental crowding, and improve his facial appearance. Cessation of the lip-biting habit was considered essential. Much attention would be given to controlling the vertical growth of his molars because of the steep mandibular plane angle.
Treatment alternatives
Our plan was 2-phase treatment. To reduce the skeletal discrepancy anteroposteriorly by growth modification, a functional appliance (Twin-block with high-pull headgear) was planned for the phase 1 treatment in preadolescence. Even though the patient did not have a posterior crossbite, it was necessary to achieve compensatory lateral expansion of the maxillary arch with a maxillary expander. We aimed to inhibit the growth of the maxilla, promote that of the mandible, and control the eruption of his molars, thus to correct the skeletal Class II relationship and improve his profile. Meanwhile, cessation of the lip-biting habit, functional training of lip muscles, and psychological counseling were important parts in the phase 1 treatment.
The need for extraction was to be determined according to the profile, the molar relationship, and other results after phase 1 treatment. A straight-wire appliance was then applied to align and level the dentition and to achieve a neutroclusion and a better profile.
Treatment progress
The Twin-block appliance was used with the maxillary expander activated once a week after an adaptation period of 2 weeks. Meanwhile, the high-pull headgear was worn for 9 months to restrict downward and forward growth of the maxilla. The patient was instructed to wear the Twin-block appliance 24 hours a day, especially during eating, and to wear the headgear at least 14 hours per day. During the phase 1 treatment, the Twin-block appliance was adjusted twice to guide the mandible forward. The patient was initially seen 10 days after the first visit, then monthly so that the blocks and the headgear could be adjusted for retention and stability as needed.
Based on the crowding and slightly convex profile after phase 1 treatment, we decided to extract the maxillary second premolars and the mandibular first premolars. Leveling and alignment progressed with nickel-titanium wires for 5 months. A lingual arch was applied to enhance anchorage during the early stage of phase 2 treatment.
An 0.018 × 0.025-in rectangular stainless steel archwire in the maxillary arch was used with T-loops to close space, and a 0.019 × 0.025-in rectangular stainless steel archwire with elastic chains was used in the mandibular arch. Meanwhile, intermaxillary traction was used to adjust the occlusion. After several adjustments of the occlusion, the fixed appliances were removed. The patient was given a pair of Hawley retainers with an inclined maxillary biteplane.
Treatment results
When the phase 1 treatment ended, the patient’s mandible was positioned forward, and the profile was greatly improved ( Fig 4 ). A skeletal anteroposterior reduction was significant with 3.8° change in the ANB angle (the SNA angle had decreased from 81.2° to 79.6°). The height of the maxillary first molar changed from 12.3 to 9 mm ( Figs 5 and 6 ; Table ). The intraoral examination showed an expanded maxillary arch, improvement of the deep overbite and large overjet, labially inclined maxillary anterior teeth, and a mesial relationship of the first permanent molars.