Orthodontic archwires or fractured appliances that are accidentally swallowed can become lodged in the airway or gastrointestinal tract. Inadvertent ingestion or aspiration of an appliance or archwire piece during orthodontic appliance adjustment is a medical emergency with potentially serious complications, including possible death from asphyxiation. This article reports the accidental ingestion of a piece of orthodontic archwire that became impacted in the larynx; it was subsequently retrieved. Some potential complications are discussed, along with suggested precautions to prevent such mishaps when using fixed appliances.
Foreign body ingestion or aspiration episodes are potential complications in all branches of dentistry. The handling of small orthodontic components in the presence of saliva demands particular care on part of the clinician, especially when the patient is supine or semirecumbent. The recent addition of microimplants to our armamentarium raises the risk of ingestion or inhalation of such components, although none has yet been reported in orthodontic literature. Accidental ingestion or aspiration of orthodontic appliances or their component parts can pose problems if they become lodged in the airway or gastrointestinal tract. It could occur during a chair-side procedure or later from inadequate retention or failure of the appliance. Such scenarios can be a medical emergency and could lead to serious complications, including possible death, from aspiration of the foreign body.
Dental literature that addresses the aspiration or ingestion of dental instruments, materials, or prostheses is replete with case reports and descriptions of adverse events. There is, however, considerable variation in the reported incidence in all published literature. In a review article, Tamura et al reported that the range varied considerably from 3.6% to 27.7% for all foreign bodies, with the number significantly higher in adults than in children. A cursory review of the pertinent literature shows that aspiration or ingestion of orthodontic appliances is less common but nonetheless varied in the types of appliances involved. Reported cases include swallowing an expansion appliance key, a mandibular spring retainer, a fragment of a maxillary removable appliance, a piece of archwire, a transpalatal arch, and a fractured Twin-block appliance. Most of these incidents, however, did not cause serious medical problems and were managed conservatively. Foreign bodies entering the alimentary canal are not a serious medical problem unless they become impacted, causing obstruction or perforation of the gut wall. Most objects will pass through without incidence. A rare case was reported of a 13-year old boy with Down syndrome who accidentally swallowed a removable quad-helix; surgical removal was necessary.
Case report
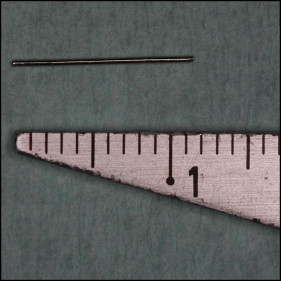
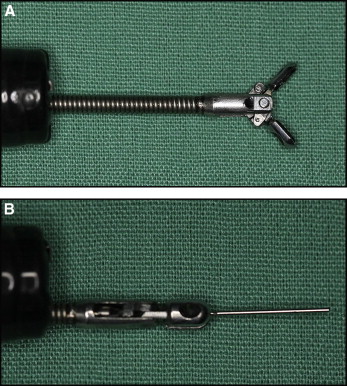
A 12-year-old girl came to the Department of Orthodontics at the National Dental Centre in Brunei, seeking orthodontic intervention for her “top front teeth” that she thought were “sticking out,” and for spacing between her mandibular teeth. Her medical history was noncontributory. She had a skeletal Class II pattern with a convex profile and mild incompetence of lips. The dental findings included features of Angle Class II Division 1 malocclusion, reduced lower facial height, missing mandibular lateral incisors, deepbite, and overjet of 7 mm. Fixed appliances (0.022-in Advant-Edge I Roth prescription brackets with a vertical slot; TP Orthodontics, LaPorte, Ind) were bonded onto both arches. A removable appliance with an anterior biteplane was also placed in the maxillary arch to relieve the deepbite. Adjustment visits proceeded uneventfully, and wire transitions were made after achieving the planned clinical stage objectives. One day, the patient arrived for an appointment feeling not quite her normal self; she was accompanied by her mother (a dental nurse). Her mother said that the girl was nervous about her upcoming examinations. Nevertheless, after reassurances, the scheduled procedures were begun, involving placing 0.018-in stainless steel archwires in both arches. After the maxillary archwire was seated, the operator proceeded to place the mandibular archwire. As the distal end was being cut, the patient suddenly jerked her head; this prompted the operator to remove the pliers from her mouth. The cut end of the wire was not in the safety hold of the pliers. The patient, who was supine during the procedure, sat up almost immediately complaining that she could feel “something sharp” in her throat. She swallowed again and said she felt “a sharp pain” in the neck region. The oral cavity and oropharynx were visually examined carefully under good illumination to rule out the possibility that the wire was entrapped in this region. No emergency treatment was attempted, since the patient did not indicate any sign of respiratory distress. Both the patient and her mother were reassured, and the possibility of her having to undergo an “endoscopy for retrieval of the wire” was outlined. Her vital signs were monitored, and the patient was immediately transferred to the hospital. Endoscopy was performed under sedation by the consultant gastroenterologist, and the archwire piece ( Fig 1 ) was retrieved from the larynx ( Fig 2 ) with a rubber tip ( Fig 3 ). The patient was discharged the same day without complications.

Discussion
This report illustrates the ease with which fixed appliance components can be swallowed or aspirated even when normal precautions are followed. This might be partly due to the miniature size and sharpness of orthodontic components, and also that the patient is usually in a supine or semirecumbent position for most orthodontic procedures. In this position, there is an increased risk of objects entering the oropharynx, although it has been suggested that a supine patient is prevented from swallowing, and hence there is a reduced risk of aspiration or swallowing of foreign bodies. Accidents, nevertheless, are possible when treating patients in either position.
Despite adequate precautions, if such events do occur, the oral cavity and the oropharynx must be carefully inspected in good light because the foreign body could be trapped in the supratonsillar recess, epiglottic vallecula, or piriform recess. If it cannot be found in these areas, it must be assumed that it has been either swallowed or aspirated. Fortunately, most foreign bodies that are ingested will enter the alimentary canal and pass through without incident, although occasionally ingestion does result in an acute medical emergency. Some of the more serious sequelae include intestinal obstruction, gut perforation with subsequent abscess formation, and hemorrhage or fistula.
When considering the potential complications of aspiration vs ingestion, the intuitive conclusion would be that aspiration is associated with a higher morbidity rate. Aspiration of a foreign body during treatment is a more serious problem that could become a life-threatening emergency. The symptoms depend on the location of the impaction in the airway. If the object becomes trapped above the level of the vocal cords, respiratory distress can warrant urgent action. Smaller objects usually do not cause obstruction and tend to pass through the vocal cords. The most common symptoms of laryngotracheal impactions are dyspnoea, cough, and stridor; bronchial foreign bodies cause coughing, decreased air entry, dyspnea, and wheezing. Hoarseness of the voice will accompany obstruction of the larynx or trachea with or without cyanosis, depending on whether the obstruction is partial or complete. Some more serious complications include bronchial stenosis, bronchiectasis, lung abcess, tissue ulceration or erosion, esophageal perforation with secondary mediastinitis, and pneumothorax. Prevention of such incidents by mandatorily following precautions aimed at securing potentially loose orthodontic objects during all procedures is probably the best approach.
The following precautions, if undertaken by the orthodontist while using fixed appliances, might help to reduce to the risk of accidental ingestion or inhalation.
- 1.
Use powder-free textured gloves to help improve the grip on instruments (and small orthodontic components such as bands).
- 2.
Tether bands with an adequate length of floss through the molar tubes during banding procedures, especially for second molars.
- 3.
Use a gauze pad as protection distal to the archwire or appliance to prevent injury to the mucosa as well as to trap any stray wires that escape the safety hold of the pliers.
- 4.
Bondable tubes have a greater risk of being inhaled or swallowed if they are dislodged, so it is advisable to cinch the archwire whenever possible.
- 5.
Periodically check the cutting tips of instruments for signs of wear or work fatigue and replace those that warrant replacement.
- 6.
Reinforce removable quad-helices and transpalatal arches at the point of attachment by using elastomeric ligatures or, preferably, stainless steel ligatures.
- 7.
During appliance debonding, it might be less risky if the brackets removed are allowed to remain attached to the base archwire.
- 8.
Microimplants must be adequately attached by steel ligatures to the main appliance through eyelets of the implant (if present). If nickel-titanium alloy springs are planned for retraction, the clinician must ensure proper attachment to the appliance.
- 9.
Visually check the cutting ends of distal cutters for trapped wires and wipe them with sterile gauze after every cut.
- 10.
For orthodontic treatment in patients with special care needs, constant monitoring of the appliance at every appointment is recommended.
- 11.
The orthodontist must ensure adequate retention and integrity of the appliance at each appointment before and after the planned adjustment.
- 12.
Advise patients, both verbally and in writing at appliance placement, that they should not try to reseat damaged, ill-fitting, or broken fragments of any appliance; instead, they should return to the orthodontist to have the appliance checked.
- 13.
Every clinic should consider the possibility of such emergencies in its standard operating procedures and be well prepared for them.
- 14.
Every orthodontist should complete a basic life support and first aid skills course. Regular updating of skills every 2 years is necessary, since the recommendations change.
Dentistry as such and orthodontics in particular pose a high risk of ingestion or inhalation of appliance components. Because of this, the orthodontist must be able to recognize the signs and symptoms of airway obstruction early if any object is lost into the oropharynx. Inability to talk and coughing forcefully with the patient’s hands clutched to the throat might be the earliest sign of choking. A partial blockage can quickly become life threatening if the patient cannot breathe properly. Complete blockage is a medical emergency. Cyanosis, loss of consciousness, and permanent brain damage occur within 4 to 6 minutes if the obstruction is not removed. Therefore, speed and updated cardiopulmonary resuscitation skills are vital on part of the clinician. If an object is inhaled and the patient shows signs of respiratory distress, attempt dislodgement with repeated sharp blows between the shoulder blades followed by abdominal thrusts (Heimlich maneuver).
If retrieval is not possible in the clinic, emergency life support measures must be initiated while waiting for help to arrive. If the airway is not compromised, the patient must be escorted to the hospital for clinical and radiographic examinations to identify the location of the object for planning the means of retrieval.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


