Since the inception of cosmetic surgery, surgeons have worked assiduously toward developing better techniques in an effort to achieve results that look more natural and unstrained. Advancements in technology sometimes provide improvements in certain aspects of a procedure without offering a better outcome. Over time, it may become apparent that older techniques performed with slight modifications ultimately can provide the best overall results in most cases. The trichophytic or modified trichal approach to forehead/brow lifting is one of those techniques.
Facial aging of the upper half of the face involves a number of features that reflect changes in various anatomic structures at different levels. These features include a retreating trichal line, thinning of follicular density, superficial rhytids and skin dyschromia, furrows, changes in brow position, and inferior positioning of infrabrow skin that causes secondary upper eyelid changes and worsening dermatochalasis of the upper lids. In some cases, genetics rather than aging plays a role in creating esthetic challenges in the periorbital region. Examples include thick infrabrow skin with a wider-than-average infrabrow shelf, intrinsically low natural upper lid creases, and thick sebaceous skin. These features may masculinize the female face.
Most skin changes, such as superficial rhytids and dyschromias, affect areas beyond the forehead region. Many of these problems can be treated dermatologically, and it would be expected that such treatments would involve all affected areas. Treatments may include chemical peels, dermabrasion, laser treatments, topicals, and, in some cases, injectable fillers. Furrows are most often muscular in nature. If furrows and creases are the only esthetic patient concerns, these can be treated by chemodenervation with agents such as botulinum toxin. Minimally invasive procedures such as barbed suture lifts have become popular in the past few years, but no long-term data have yet been gathered regarding the length of expected outcomes for these procedures.
When features of aging that affect the upper half of the face are severe enough to affect the periorbital area, surgical procedures may be required if less invasive procedures such as injection and resurfacing are not adequate. The constellation of forehead/brow procedures has included coronal lifts, trichal lifts, trichophytic (modified trichal) lifts, mid-forehead lifts and direct brow lifts. Each of these approaches has enjoyed popularity at different points in time; some have fallen into and out of favor over the past several decades. Each has its potential advantages and pitfalls ( Table 27-1 ).
| Procedure Type | Incision Location | Supposed Advantage(s) | Disadvantage(s) |
|---|---|---|---|
| Coronal lift | Over coronal scalp |
|
|
| Trichophytic | 5 mm cephalad to trichal line |
|
|
| Mid-forehead | In forehead furrow(s) |
|
|
| Direct | At cephalad margin of brow |
|
|
| Endoscopic | Multiple incisions behind trichal line |
|
|
Selection of which technique or techniques to use should be based first on careful identification of which specific features contribute most to the displeasing esthetic concern expressed by the patient.
Next, the procedure that is selected should grant the surgeon access to the areas that need correction while leaving the least noticeable signs that an operation has been performed. It is this second statement that has probably driven endoscopic techniques toward great popularity in that they were developed to be, and have have been touted as, “minimally invasive” because smaller entry sites are used for instrumentation. As soon will become apparent, this “minimally invasive” moniker is fallacious in that endoscopic techniques require disruption of anatomy that can and often should be avoided through the use of other techniques.
Forehead/brow lift techniques such as the coronal lift, the mid-forehead lift, and the direct lift are discussed in greater detail in other chapters.
THE ENDOSCOPIC BROW LIFT
These techniques are based on the concept of being minimally invasive in that the incisions are smaller, although in some cases they may be numerous. However, it is important to note that the lift achieved by sliding the forehead coronally over the access sites must stretch the scalp toward and beyond its vortex. In this way, the distance from the brow to the trichal line will be lengthened. This is one of the major disadvantages of this technique in that forehead lengthening is one of the primary features of facial aging.
Additionally, although access to the subgaleal or the subperiosteal plane may be gained through smaller incisions, the area that requires dissection is significant in that the scalp must slide over the cranium toward the occiput. Not only does this make the procedure not a minimally invasive procedure, it also increases the risk of postoperative hematoma formation. Although this risk may be considered a small one, it is a risk that must be considered because intervention would be required.
Fixation techniques for endoscopic lifts vary from surgeon to surgeon. The two most common fixation techniques are periosteal suture fixation and cranial screw anchoring. Because fixation points are focal and small with either technique, the likelihood of soft tissue relapse or alopecia is increased over the areas of fixation. Relapse is likely due to connective tissue relaxation and remodeling over time. Alopecia most likely results from diminished blood flow to the subdermal and dermal vascular complexes in an area that is placed under greater tension during healing. Often, alopecia does not become evident until several months postoperatively.
THE TRICHOPHYTIC BROW LIFT
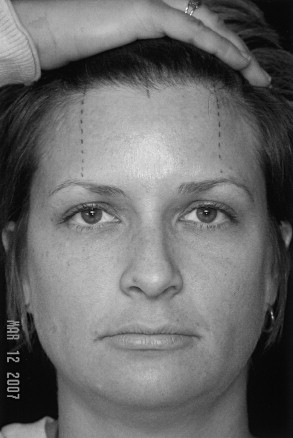
The trichophytic forehead/brow lift technique requires an incision that is near the hairline; provides direct access to the subcutaneous, subgaleal, or subperiosteal plane; is performed close enough to the supraorbital rim to allow the surgeon access for accurate lifting; provides a means by which to visualize the supraorbital and supratrochlear nerves for avoidance of injury; and is one of the most versatile of the techniques that are currently available to address brow and forehead asymmetries. Different from coronal and endoscopic techniques, this approach preserves but does not lengthen the forehead. This fact is important not only in females but also in males, who may be facing previous androgenically induced trichal retreat. Although this technique requires an incision of some significant length, it can be performed in a way that minimizes the risk of creating areas of alopecia, which is often seen with other techniques, and it typically heals in a way that is impressively inconspicuous owing, in part, to the incision design and location. This combination of factors makes this technique one of the most versatile, safe, and reliable procedures for esthetic rejuvenation of the upper half of the face ( Figures 27-1, 27-2, and 27-3 ).


SURGICAL TECHNIQUE FOR THE TRICHOPHYTIC FOREHEAD/BROW LIFT
In the preoperative area, the patient is marked in a sitting position. The region of the brow that is to receive the greatest lift and/or apex of the arch is identified, and a vertical mark is drawn to and across the trichal line. The midline also is marked across the trichal line for reference. The author uses a permanent black laundry marking pen so that moisture generated during the procedure will not displace the ink. It quickly becomes apparent that although the ink may be permanent on laundry, it is temporary on skin.
The hair is combed toward the scalp vertex and approximately 5 to 7 mm behind the trichal line; the surgical marking pen is used to delineate the incision site. It is important to ensure that the incision entry site is at least 5 to 7 mm caudal to the trichal line because the incision will be a very shallow, beveled incision that is specifically designed (1) to incise through hair shafts as it extends down toward and through the dermis, but (2) to stay ABOVE existing follicles, leaving them intact. These follicles will give rise to new hair that eventually will grow right through the incision site itself, further hiding the incision. Additionally, this technique avoids damage to the hair follicles, which fade in density at the leading edge of the trichal line (the important 5 to 7 mm zone described earlier). This allows the more natural appearing hairline that is produced through this technique.
As the incision marking line is extended laterally to the area directly above the lateral-most extension of the natural brow, it may be curved back farther into the pretemporal region. This portion of the incision will be transitioned into one that is parallel with hair follicles. This is acceptable in this region because although some small amount of tissue may be excised in this region, closure will require no tension whatsoever. Therefore, a “butt joint” type of reapproximation is favorable, and no alopecia should result as long as the surgeon avoids cautery of incision edges that could damage hair follicles. Once the incision lines are marked and pigtails are placed, the patient is brought to the operating room for the procedure. The author prefers to perform these procedures with IV sedation and local anesthesia because this allows for intraoperative facial animation and a more natural facial muscle tone during surgery. Once the appropriate level of IV sedation has been achieved, supraorbital nerve blocks are administered, typically with 1.0 to 1.5 mL of 1% lidocaine with 1 : 100,000 epinephrine. The incision line then is injected with the same solution. The patient is prepped and draped for the procedure.
The assistant is instructed to put significant tension across the incision line, so the skin is taut. A No. 11 blade is used to incise the skin with a very shallow bevel, with the tip of the blade extending to just beyond the most anterior follicles as it dives from skin surface to subdermal fat. This shallow, beveled incision is carried from the left lateral brow extension of the incision marking to the right. On each side, extending farther laterally, a No. 15 blade is used; it is transitioned perpendicular to the skin surface and thereby parallels hair follicles. Once in the subdermal fat, face-lift of Metzenbaum scissors may be used to dissect down to the planned level for flap elevation. The author prefers a subgaleal approach in most cases. Once the subgaleal plane has been entered, elevation of the flap in this avascular plane progresses quickly.
As dissection in the subgaleal plane approaches the supraorbital rim, wooden-handled cotton swabs can be used to sweep until the supraorbital and supratrochlear nerve trunks can be seen. An incision then can be made caudal to the nerve trunks, parallel to the supraorbital rims, to allow for subperiosteal dissection toward the rim prominence itself. This release provides favorable mobility for brow lifting as needed.
The surgeon may directly transect frontalis, corrugator and procerus muscle fibers as desired through the subgaleal approach. This can be done to decrease muscular furrowing. Care must be taken to avoid disruption of the subdermal vascular complex or thinning of tissue to an excessive degree, both of which can lead to scar formation or skin sloughing.
Bipolar cautery is used carefully for point hemostasis when needed. It is important to avoid cauterization near hair follicles to prevent alopecia in those areas. Allis clamps are placed on the forehead flap margin at the edge directly above the planned apex of the brow arch, which should be found easily because of preoperative marking with the permanent laundry marker. Lifting can be applied with the Allis clamps, and adjustments made to achieve the planned amount of lift. If two Allis clamps are used on each side, a back cut with surgical scissors then can be made between the clamps so that temporary staples can be placed. The assistant pushes the cephalic portion of the scalp toward the brow, and the surgeon lifts the forehead flap under moderate tension toward the coronal scalp margin, stapling at the junction points at the apex of the back cuts. Then, the surgeon and the assistant can let go and recheck to see that the appropriate amount of lift has been achieved with favorable symmetry. Adjustments can be made as needed.
Once it has been decided that the correct amount of lift has been achieved, the more tedious portion of the procedure can commence. The next phase of the operation is to trim the flap, carefully reapproximate the galea and frontalis, and perform meticulous subcutaneous closure and skin closure. It is essential that a shallow bevel be used to trim the overlapping forehead edge of the flap to match the caudad margin of the flap, so that when they are laid against each other, they create an ideal match. Use of new scalpel blades is recommended so that clean incisions can be made. After the beveled portion of the flap is addressed, the lateral areas can be trimmed with a No. 15 scalpel. After flap margins have been trimmed appropriately, closure of the galea and frontalis can proceed. The author uses 4-0 polyglycolic suture. Temporary staples then can be removed, and closure in those areas can be completed. Subcutaneous closure is performed with the use of 5-0 polyglycolic suture. Skin closure is achieved, typically in a running fashion with the use of 5-0 or 6-0 monofilament nylon suture. Bacitracin ointment is applied to the incision sites, telfa pads are placed over the incisions followed by fluffed 4 × 4’s, and a self-adhesive ACE-type bandage is applied gently.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


