Many dentofacial deformities require surgery to both the maxilla and the mandible to optimize occlusal function, facial esthetics, and stability of the results. Conventional treatment planning in double-jaw surgery either maintains the existing occlusal plane angulation or alters it by rotation of the mandible after vertical repositioning of the maxilla (superiorly or inferiorly). Although treatment according to these designs may achieve an acceptable relationship of the teeth in centric relation, it may on occasion not provide for optimum esthetics.
The correction of most dentofacial deformities requires single-jaw surgery whereby either the mandible or the maxilla is repositioned. Repositioning the mandible may involve advancement or setback, and this horizontal movement should take place along the occlusal plane of the maxilla (the unoperated jaw). Maxillary repositioning, either anteriorly or posteriorly (albeit seldom), will also take place along the existing occlusal plane. The maxilla, however, may also be repositioned superiorly, for the correction of vertical maxillary excess, or inferiorly, for the correction of vertical maxillary deficiency. A change in the anterior facial height has a significant effect on the horizontal relationship of the jaws as a result of forward or backward rotation of the mandible. Altering the height of the maxilla gives rise to rotation of the mandible, either counterclockwise (after superior repositioning of the maxilla) or clockwise (after downgrafting of the maxilla) around a point at or just posterior to the mandibular condyle. The final occlusal plane will therefore be determined by the mandibular occlusal plane after autorotation. Adhering to conventional treatment methods (especially in very high or low occlusal plane angle cases) may hamper achievement of optimal esthetic results. These limitations on the esthetic outcome can, however, be overcome by rotation of the maxillomandibular complex, also known as alteration or manipulation of the occlusal plane. The alteration should not be considered an attempt to change or treat an abnormal occlusal plane angle to a more cephalometrically normal angle.
Surgery to both jaws allows the surgeon to alter the occlusal plane angulation and effectively rotate the lower face (the maxillomandibular complex) in either a clockwise or counterclockwise direction to enhance the esthetic outcome. The facial types that would benefit most from rotation of the maxillomandibular complex are the high occlusal plane, leptoprosopic, dolichocephalic facial type and the low occlusal plane, euryprosopic, brachycephalic facial type. However, small rotations and occlusal plane alterations may often benefit patients with less severe occlusal plane angles.
The anteroposterior spatial relationship of the jaws relative to the nasion is influenced by the anterior cranial base length, the steepness of the cranial base, and the occlusal plane angle. The profound effect that a high occlusal plane angle may have on the relationship of the apical bony base of the maxilla and the mandible to the skull base and to each other is demonstrated in Figure 12-1 . The occlusal plane should therefore always be an important consideration in orthognathic diagnosis and surgical treatment planning.
GEOMETRY AND PLANNING OF THE ROTATION OF THE MAXILLOMANDIBULAR COMPLEX
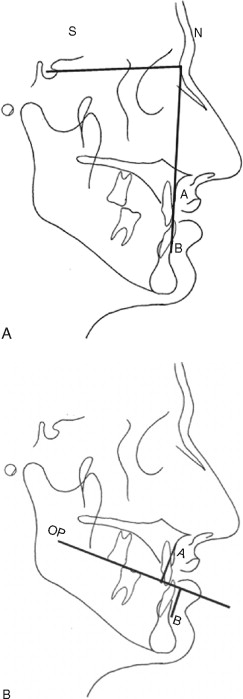
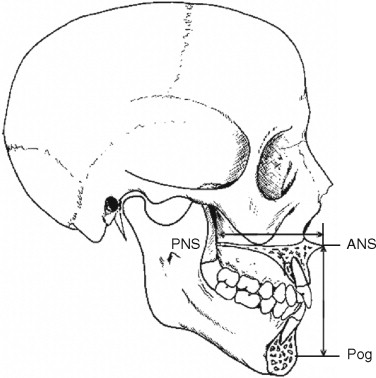
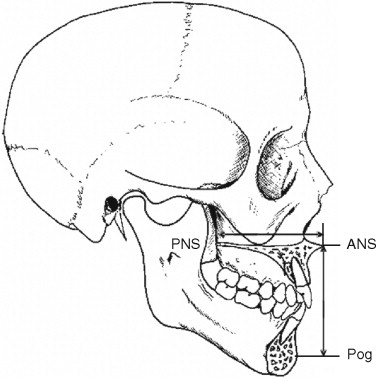
When two-jaw surgery is planned and performed, the final horizontal and vertical relationship among the anterior nasal spine (ANS), the maxillary incisor edge, and pogonion (Pog) are key determinants of esthetic outcome. The horizontal interrelationship among ANS, the upper incisor tip, and Pog is a consequence of the horizontal dental and skeletal relationships, that is, Class I, Class II, or Class III. At the same time the vertical relationship among ANS, the upper incisor tip, and Pog are influenced by the vertical skeletal and dental pattern, that is, the vertical maxillary deficiency, vertical maxillary excess, and deep or open bite.
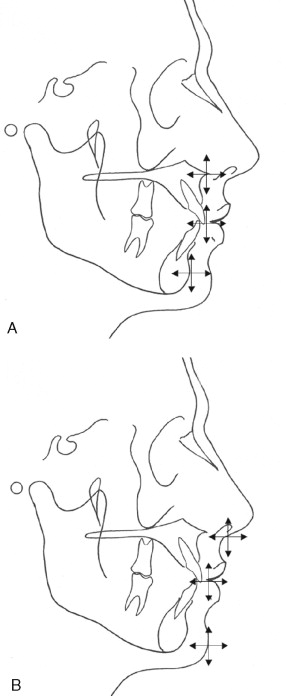
The interrelationship of important soft-tissue landmarks such as the subnasale (Sn), upper lip position (and its relationship to maxillary incisor), and Pog are directly dependant on the position of underlying skeletal and dental structures (ANS, upper incisor, and Pog, respectively) ( Figure 12-2 ).
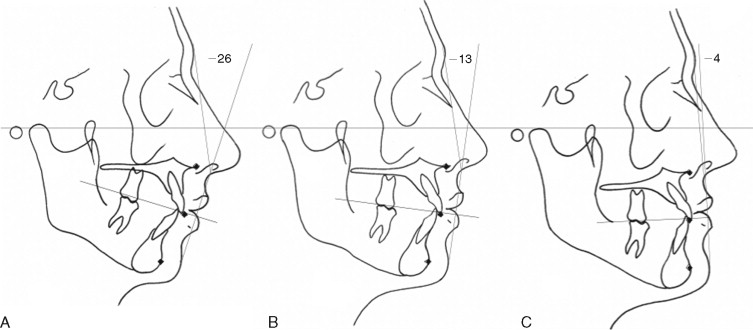
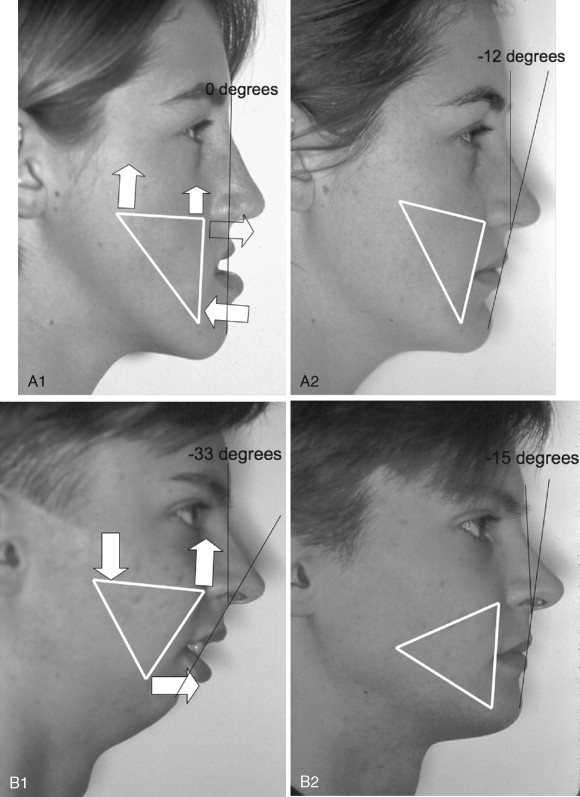
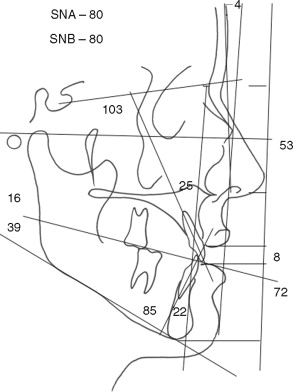
In some hyperdivergent and hypodivergent cases, the hard-tissue landmarks ANS, incisor tip, and Pog may be well related to one another; however, the patient may still have an excessively convex or concave profile. The interrelationship of the above hard-tissue landmarks is identical in Figure 12-3 ; however, owing to the difference of the occlusal plane angle, the profiles differ substantially.
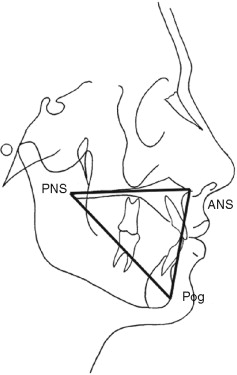
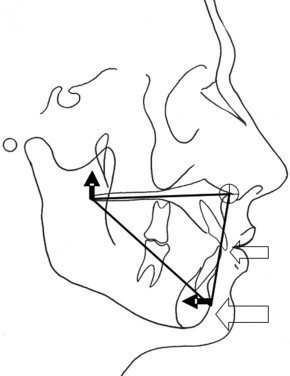
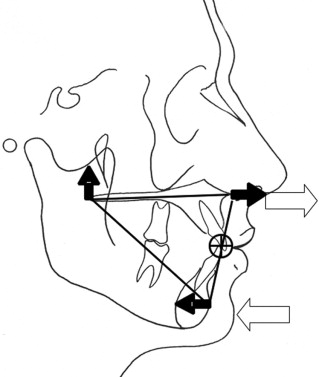
For visualization of treatment options and hard- and soft-tissue changes subsequent to surgical repositioning of the maxilla and mandible independent of the existing occlusal plane, a triangle is constructed. A cephalometric tracing of a patient with relatively normal soft-tissue and skeletal relationship and a Class I occlusion is demonstrated in Figure 12-4 . The triangle is constructed by connecting the ANS, posterior nasal spine (PNS), and Pog and is called the maxillomandibular triangle.
The cephalometric tracing (with the constructed maxillomandibular complex triangle) is used to investigate various soft-tissue and hard-tissue changes that can be expected by rotating the maxillomandibular complex in a clockwise direction (increasing the occlusal plane angle) or counterclockwise (decreasing the occlusal plane angle). The varied soft-tissue, skeletal, and dental changes obtainable by rotating the maxillomandibular complex around different points are shown, and clinical cases in which this concept is used, are demonstrated.
THE LINEAR DIMENSIONS BETWEEN PNS-ANS AND ANS-POG
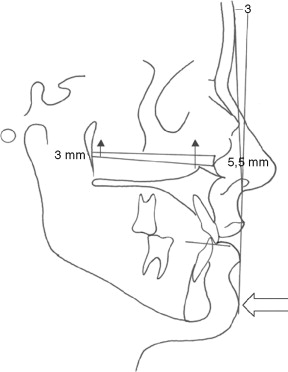
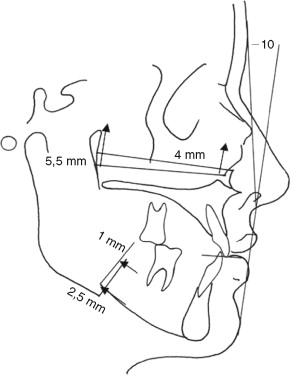
The maxillary length (PNS-ANS) forms the horizontal leg of the maxillomandibular triangle, whereas the vertical facial height (ANS-Pog) forms the vertical leg ( Figure 12-5 ). In a study of 40 dry skulls, Reyneke found that the average maxillary length was 47.6 mm and the average facial height measured 66.5 mm. The fact that the horizontal leg of the triangle is shorter than the vertical leg enables the clinician to use a “gearing” effect during rotation of the triangle. A small change in the angulation of the horizontal leg will result in a larger change in the vertical leg.
THE LINEAR DIMENSIONS BETWEEN PNS-ANS AND ANS-POG
The maxillary length (PNS-ANS) forms the horizontal leg of the maxillomandibular triangle, whereas the vertical facial height (ANS-Pog) forms the vertical leg ( Figure 12-5 ). In a study of 40 dry skulls, Reyneke found that the average maxillary length was 47.6 mm and the average facial height measured 66.5 mm. The fact that the horizontal leg of the triangle is shorter than the vertical leg enables the clinician to use a “gearing” effect during rotation of the triangle. A small change in the angulation of the horizontal leg will result in a larger change in the vertical leg.
GEOMETRY OF THE TREATMENT DESIGN USING THE CONSTRUCTED MAXILLOMANDIBULAR TRIANGLE
The correction of a Class III dentofacial deformity requiring surgery to both jaws will involve maxillary advancement combined with mandibular setback. Rotation of the maxillomandibular complex in a clockwise direction will, however, increase the facial contour angle and enhance the correction, whereas counterclockwise rotation will decrease the facial contour angle and temper the correction ( Figure 12-6 ).
The surgical correction of the severe convex profile in Figure 12-6, B will require maxillary superior repositioning and mandibular and chin advancement. Counterclockwise rotation of the maxillomandibular complex will enhance the mandibular advancement and reduce the need for excessive advancement of the chin.
The center of rotation around which the maxillomandibular complex can be rotated may be located at ANS, the tip of the maxillary incisor tooth, PNS, the zygomatic buttress, or Pog. The selection of the direction of rotation and the point of rotation is dictated primarily by the esthetic requirements of each case.
The following text, tables, and figures illustrate the basic skeletal, dental, and soft-tissue changes that can be expected with clockwise and counterclockwise rotation of the maxillomandibular complex as well as the subtle differences in results that can be achieved by changing the rotation point.
CLOCKWISE ROTATION OF THE MAXILLOMANDIBULAR COMPLEX
CENTER OF ROTATION AT ANS
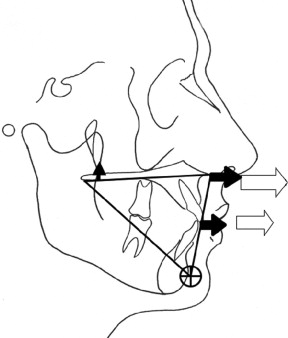
Surgical superior repositioning of the posterior maxilla as a result of rotation around ANS will result in the changes illustrated in Figure 12-7 and summarized in Table 12-1 . The extent of posterior repositioning of Pog is greater than the amount of superior repositioning of the posterior maxilla owing to the fact that the anterior height of the maxillomandibular triangle (ANS-Pog) is greater than the anteroposterior length of the maxilla (ANS-PNS).
| Hard-Tissue Changes | Soft-Tissue Changes | ||
|---|---|---|---|
| OP angle | Increase | Subnasale | Advance |
| Maxillary incisor tip | No change | Upper lip support | No change |
| Pog position | Set back | Facial convexity (contour) | Increase |
| Upper incisor angle | Decrease | Mandibular prominence | Decrease |
| Maxilla at ANS | Advance | Paranasal fullness | Increase |
| MP angle | Increase | Nasolabial angle | Increase |
| Posterior maxillary height | Decrease | Anterior facial height | No change |
| Chin throat length | Decrease | ||
* A summary of the expected hard- and soft-tissue changes after clockwise rotation of the maxillomandibular complex, which are shown in Figure 12-7 .
CENTER OF ROTATION AT THE MAXILLARY INCISOR TIP
Surgical superior repositioning of the posterior maxilla as a result of clockwise rotation of the maxilla around the maxillary incisor tip will result in the changes illustrated in Figure 12-8 and summarized in Table 12-2 .
| Hard-Tissue Changes | Soft-Tissue Changes | ||
|---|---|---|---|
| OP angle | Increase | Subnasale | Advance |
| Maxillary incisor tip | No change | Upper lip support | No change |
| Pog position | Set back | Facial convexity (contour) | Increase |
| Upper incisor angle | Decrease | Mandibular prominence | Decrease |
| Maxilla at ANS | Advance | Paranasal fullness | Increase |
| MP angle | Increase | Nasolabial angle | Increase |
| Posterior maxillary height | Decrease | Anterior facial height | No change |
| Chin throat length | Decrease | ||
* The hard- and soft-tissue changes that may be expected after the rotation of the maxillomandibular complex in a clockwise direction around the tip of the maxillary incisor tooth are summarized in this table and illustrated in Figure 12-8 .
The ratio of the extent of the anterior movement of ANS to the posterior movement of Pog is the same as the ratio of the distance from ANS to the tip of the maxillary central incisor to the distance from the tip of the incisor to Pog.
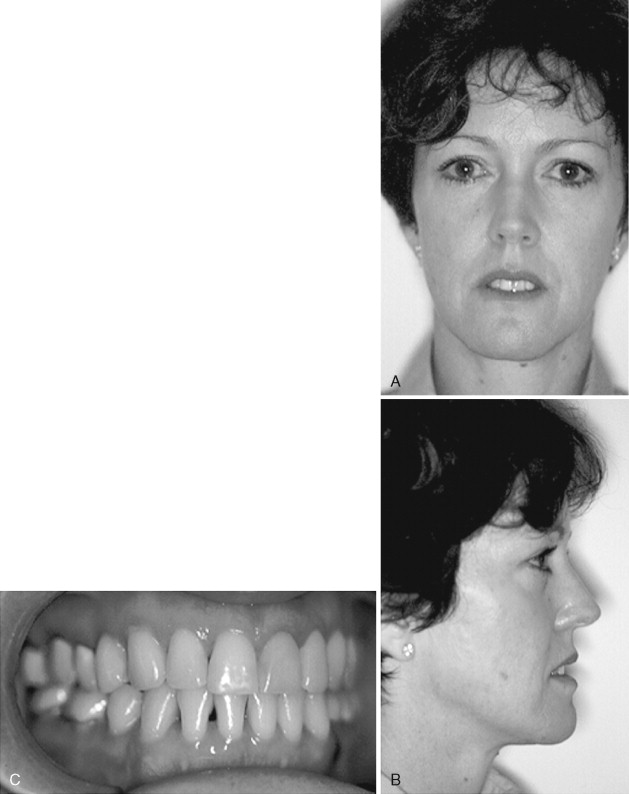
This patient was unhappy about the strong appearance of her lower jaw and lip incompetence after her orthodontic treatment. Her maxilla was vertically excessive and the mandible anteroposteriorly excessive. The orthodontic treatment consisted of the extraction of the lower first bicuspids, and a Class I occlusion (Class III molar relationship) was established ( Figures 12-9 and 12-12, A through C ). The occlusion limited any surgical correction by conventional treatment methods unless dental decompensation was attempted by further orthodontic treatment. Conventional surgical treatment would consist of vertical reduction of the maxilla and anteroposterior reduction of the chin by genioplasty. The autorotation of the mandible would increase the prominence of the mandible, whereas a reduction genioplasty would obliterate the labiomental fold ( Figure 12-10 ). This treatment option would certainly worsen the esthetics. Through performance of double-jaw surgery, rotating the maxillomandibular complex in a clockwise direction around the incisor tip, the existing occlusion could be maintained, while the chin contour would also not change ( Figure 12-11 ). The treatment result performed by using the rotation of the maxillomandibular complex design (see Figure 12-11 ) is illustrated in Figure 12-12, D and E .
FLOAT NOT FOUND

CENTER OF ROTATION AT POGONION
Clockwise rotation of the maxillomandibular complex around Pog will result in the hard- and soft-tissue changes illustrated in Figure 12-13 and summarized in Table 12-3 .
| Hard-Tissue Changes | Soft-Tissue Changes | ||
|---|---|---|---|
| OP angle | Increase | Subnasale | Advance |
| Maxillary incisor tip | Advance | Upper lip support | Increase |
| Pog position | No change | Facial convexity (contour) | Increase |
| Upper incisor angle | Decrease | Mandibular prominence | No change |
| Maxilla at ANS | Advance | Paranasal fullness | Increase |
| MP angle | Increase | Nasolabial angle | Increase |
| Posterior maxillary height | Decrease | Anterior facial height | No change |
| Chin throat length | Decrease | ||
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


