A girl, aged 11 years 4 months, with a skeletal Class II pattern and a severe overjet (10 mm) was treated with a Twin-block appliance. After 9 months of appliance therapy, the skeletal Class II was overcorrected. After 26 months of retention, when the occlusion was stable and the growth rate was diminishing, fixed orthodontic appliances using temporary skeletal anchorage devices were initiated. The total active treatment time with fixed orthodontic appliances was 30 months. Posttreatment records after 18 months demonstrated excellent stability: a functional occlusion and a pleasing facial balance. Cone-beam computed tomography was used to visualize temporomandibular joint adaptations after the functional and fixed orthodontic therapies.
Highlights
- •
A growing girl had a Class II malocclusion, severe overjet, and retrognathic mandible.
- •
She was treated with a Twin-block and fixed appliances.
- •
Functional therapy was done during a period of peak growth.
- •
CBCT images showed that joint space between condyle and glenoid fossa was normalized.
When a Class II malocclusion is due to a retrognathic mandible, positioning the mandible forward is believed to enhance its growth. To correct a Class II skeletal pattern and a malocclusion, functional appliances have been widely used. Placement of a functional appliance results in displacement of the condyle in the glenoid fossa, stimulates growth of the condylar cartilage, and induces an accompanying lengthening of the mandible. The primary purpose of functional appliances such as the Twin-block is to modify or redirect mandibular growth to correct a skeletal discrepancy.
It has been reported that the efficiency of treatment of a retrognathic mandible strongly depends on the biologic responsiveness of the condylar cartilage. During functional appliance treatment, changes in the mandibular condyle relative to mandibular advancement highly depend on the duration of functional therapy plus the direction, amount, and types of forces used. However, it is still undetermined whether growth modification increases the total amount of mandibular growth or whether it only increases the rate of the genetically predetermined amount of mandibular growth.
This article demonstrates successful orthodontic treatment using a Twin-block appliance and fixed orthodontic treatment for a girl who was 11 years 4 months of age with a severe skeletal Class II overjet (10 mm) caused by a retrognathic mandible. A normal occlusion and an improved profile were achieved after treatment. The use of cone-beam computed tomography (CBCT) allowed us to visualize the temporomandibular joint (TMJ) adaptations after functional therapy and fixed orthodontic treatment.
Diagnosis and etiology
The girl was referred for an evaluation of orthodontic treatment. Her chief complaint was protrusion of her maxillary anterior teeth. The patient had a mesiofacial pattern and a Class II appearance. She had a protrusive upper lip, and when her lips touched in a rest position, she had lip strain. There was no significant facial asymmetry.
Intraorally, she had proclined maxillary anterior teeth with a 10-mm overjet and a 30% overbite. She showed end-on Class II molar and canine relationships on both sides. She had moderate crowding in both arches, and her mandibular right permanent second premolar was emerging. She also had a deep curve of Spee of her mandibular arch. Her maxillary dental midline was coincident with her facial midline, and the mandibular dental midline deviated 0.5 mm to the right ( Figs 1 and 2 ).

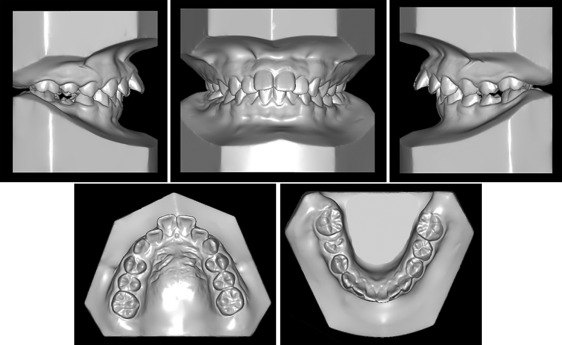
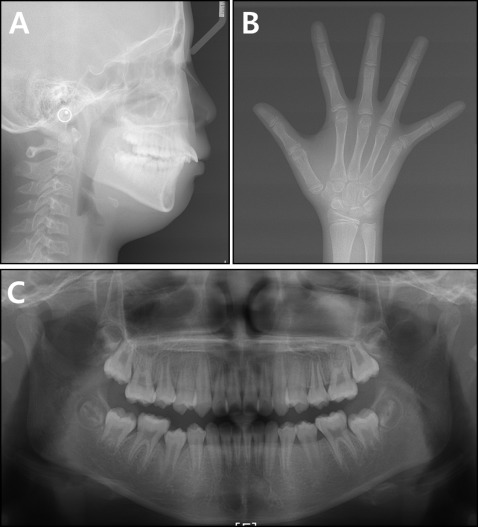
A panoramic radiograph showed a slight difference between her right and left condylar heads. However, during TMJ evaluation, she did not report any muscle pain, joint pain, or other symptoms typically associated with temporomandibular disease. All third molar buds could be seen on the radiograph.
The lateral cephalometric analysis indicated a skeletal Class II pattern (ANB, 6.3°) with a hyperdivergent growth pattern (SN-MP, 37.5°). The maxillary and mandibular incisors were proclined (U1 to SN, 113.5°; IMPA, 96.6°) ( Fig 3 ; Table I ).
| Measurement | Norm | T1 | T2 | T3 | T4 | T5 | T6 |
|---|---|---|---|---|---|---|---|
| SNA (°) | 82.0 | 80.2 | 79.2 | 79.9 | 80.1 | 79.4 | 79.5 |
| SNB (°) | 79.9 | 73.9 | 75.8 | 77.8 | 77.5 | 76.2 | 76.2 |
| ANB (°) | 2.1 | 6.3 | 3.4 | 2.1 | 2.6 | 3.2 | 3.3 |
| Wits (mm) | 1.1 | 0.2 | −5.8 | −8.2 | −5.9 | −4.5 | −4.2 |
| SN-MP (°) | 34.0 | 37.5 | 37.9 | 37.3 | 37.0 | 37.6 | 36.6 |
| FH-MP (°) | 28.2 | 28.4 | 29.2 | 28.5 | 26.8 | 28.5 | 27.6 |
| LFH (ANS-Me/N-Me) (%) | 55.0 | 52.0 | 54.0 | 55.0 | 54.0 | 54.0 | 54.0 |
| U1-SN (°) | 104.0 | 113.5 | 99.2 | 101.3 | 110.0 | 101.1 | 101.3 |
| U1-NA (°) | 22.0 | 33.3 | 20.0 | 21.5 | 29.9 | 21.8 | 21.8 |
| IMPA (°) | 90.0 | 96.6 | 102.3 | 97.0 | 96.5 | 98.0 | 98.2 |
| L1-NB (°) | 25.0 | 27.9 | 35.9 | 32.1 | 31.0 | 31.7 | 31.0 |
| U1/L1 (°) | 124.0 | 112.5 | 120.8 | 124.4 | 116.5 | 123.3 | 123.9 |
| Upper lip (mm) | 1.2 | 4.4 | 0.5 | 0.6 | 2.0 | 1.3 | 0.8 |
| Lower lip (mm) | 2.0 | 3.4 | 2.3 | 1.7 | 3.2 | 1.8 | 1.3 |
Treatment objectives and plan
The following treatment objectives were established: (1) improve the patient’s skeletal Class II pattern, (2) improve her profile, (3) establish Class I canine and molar relationships, (4) obtain normal overjet and overbite, (5) relieve the crowding in both arches, (6) level the curve of Spee, (7) obtain a stable occlusal relationship, and (8) improve facial and dental esthetics by establishing an esthetic smile.
Since the patient was still growing, the initial treatment objective was to reduce her overjet by skeletal improvement, thus promoting mandibular growth. If functional appliances could reposition mandibular growth forward and improve overjet, nonextraction or extraction could be considered for the next stage of treatment. Details of this treatment plan were presented to the patient and her mother. They elected to use the Twin-block appliance to promote mandibular growth and then consider fixed orthodontic treatment after functional appliance therapy.
Treatment objectives and plan
The following treatment objectives were established: (1) improve the patient’s skeletal Class II pattern, (2) improve her profile, (3) establish Class I canine and molar relationships, (4) obtain normal overjet and overbite, (5) relieve the crowding in both arches, (6) level the curve of Spee, (7) obtain a stable occlusal relationship, and (8) improve facial and dental esthetics by establishing an esthetic smile.
Since the patient was still growing, the initial treatment objective was to reduce her overjet by skeletal improvement, thus promoting mandibular growth. If functional appliances could reposition mandibular growth forward and improve overjet, nonextraction or extraction could be considered for the next stage of treatment. Details of this treatment plan were presented to the patient and her mother. They elected to use the Twin-block appliance to promote mandibular growth and then consider fixed orthodontic treatment after functional appliance therapy.
Treatment alternatives
With growth modification possible, the patient’s Class II malocclusion could be corrected by either nonextraction or extraction treatment after functional therapy. However, since her maxillary incisors were excessively proclined, total arch distalization of the maxillary arch using temporary skeletal anchorage devices (TSADs) plus vertical control of the maxillary first molars could induce counterclockwise rotation of the mandible and improve the skeletal Class II pattern.
The other treatment option was to extract the maxillary first premolars and finish the patient with Class II molar and Class I canine relationships. Additionally, extraction of the maxillary first premolars and the mandibular second premolars was discussed to correct the Class II malocclusion.
Because her skeletal discrepancies resulted from an unfavorable Class II skeletal growth pattern, the possibility of 1-jaw or 2-jaw surgery after completion of growth was also discussed. Upon completion of the orthodontic treatment, a genioplasty was suggested to improve her profile, but the family declined all surgical options.
Treatment progress
Before orthodontic treatment, the patient was referred to a general dentist to verify that she had no caries. Treatment began with a modified Twin-block appliance originally developed by Clark ( Fig 4 ). Jaw registrations showed approximately 10 mm of protrusion, and the blocks were 3 to 4 mm apart in the buccal segment. The steep inclined planes interlocked at about 7° to the occlusal plane. The appliance was adjusted once per month for approximately 9 months. During adjustment, acrylic was progressively removed from the undersurface of the posterior bite-blocks to allow for the eruption of the mandibular molars; this helped to level the curve of Spee. The patient was instructed to wear the appliance 24 hours a day, including at mealtimes.

To prevent relapse, the Class II dental relationships, severe overjet, and deep overbite were overcorrected ( Figs 5 and 6 ). During the retention stage, a maxillary modified Hawley retainer with an anterior inclined plane was worn at night for 12 months ( Figs 7-9 ). A 3-month recall schedule was maintained to evaluate the occlusion and growth, and guide the condyle into a natural position without a retainer ( Figs 10 and 11 ). After 26 months of retention (age, 14 years, 3 months), 0.022 × 0.028-in standard edgewise appliances were placed in both arches. Leveling of the dentition began with a 0.014-in nickel-titanium archwire, followed by an 0.018-in nickel-titanium archwire, and ended with a 0.017 × 0.025-in stainless steel archwire.


