This case report describes the orthodontic treatment of a girl who lost her maxillary left central incisor from trauma. The patient had a concave profile, a Class I molar relationship on the right side and a Class II molar relationship on the left side, with a slight maxillary retrusion, an anterior edge-to-edge bite, and a posterior crossbite. Therefore, the treatment consisted of rapid palatal expansion to widen the maxilla in a transverse direction along with reverse headgear to improve the incisor relationship. The crown of the left canine was modified to resemble the left lateral incisor, and a porcelain veneer was placed to make the left lateral incisor resemble the left central incisor. This case report illustrates how orthodontics alone can be used to treat a missing central incisor, without a bridge or an implant.
Traumatic loss of maxillary incisors during the active teenage years is a serious and challenging clinical situation. Because of the frequency of dental trauma in infancy and childhood, traumatized teeth with various long-term prognoses pose a problem when planning orthodontic treatment. An orthodontist often becomes involved in managing these patients because of accompanying malocclusions such as midline shift, anterior crossbite caused by space loss, or ectopic eruption of adjacent teeth.
The alternative approaches include reimplantation of the avulsed tooth, autotransplantation, placement of a bridge or an implant during adulthood, and substitution of the ipsilateral lateral incisor for the central incisor after space closure. The choice of the appropriate solution for the missing maxillary central incisor depends on the specific characteristics of each situation. However, the success of reimplantation depends on the status of the tooth’s root, the ability to perform endodontics, and the length of time that the tooth has been out of the alveolar socket. Some adolescents whose roots are not completely formed should not have restorations.
This case report describes the orthodontic treatment of a patient who was missing a maxillary central incisor because of trauma; the treatment was completed without placing a bridge or an implant.
Diagnosis and etiology
This girl had avulsed her maxillary left central incisor when she was 8 years old. Although the tooth was retrieved at that time, the patient did not see a dentist to treat the trauma. At 14 years of age, she became concerned about the esthetic appearance of her teeth and facial profile and wanted orthodontic treatment. At that age, all permanent teeth had erupted, and the edentulous space had closed entirely.
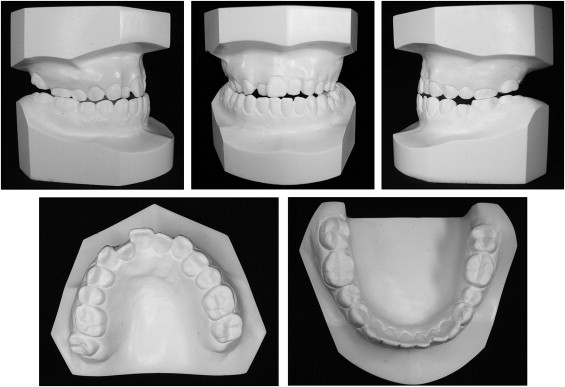
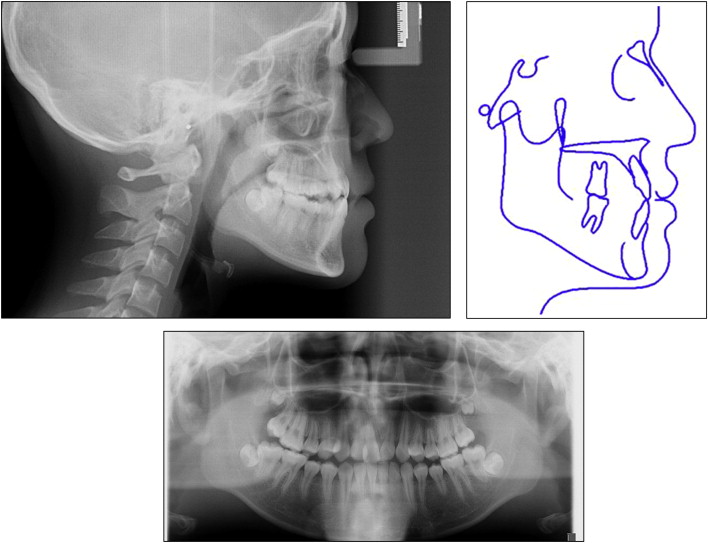
Viewed from the front, her face was well balanced and symmetric. Her facial profile was concave, with a slight maxillary retrusion and normal vertical proportions. No signs or symptoms of any temporomandibular joint disorder were noted.
Intraorally, she had a mild Angle Class I molar and premolar relationship on the right side and an Angle Class II molar and premolar relationship on the left side. She had an anterior edge-to-edge bite and a posterior crossbite combined with palatal transversion and crossbite of the maxillary right lateral incisor.
The maxillary dental midline deviated by 2.0 mm to the left with respect to the facial midline because of the missing central incisor. The mandibular dental midline was almost coincident with the facial midline. She had mild crowding of the maxillary and mandibular arches ( Figs 1-3 ).

Treatment objectives
The primary treatment objectives were to restore the normal appearance of the maxillary anterior teeth and establish an acceptable occlusion despite the missing central incisor. The other essential objectives were to protract and expand the maxilla to correct the maxillary deficiency and the posterior crossbite. Ideal overbite relationships were also desirable to establish immediate anterior guidance. Additional objectives were to eliminate the crowding and correct the maxillary dental midline.
Treatment objectives
The primary treatment objectives were to restore the normal appearance of the maxillary anterior teeth and establish an acceptable occlusion despite the missing central incisor. The other essential objectives were to protract and expand the maxilla to correct the maxillary deficiency and the posterior crossbite. Ideal overbite relationships were also desirable to establish immediate anterior guidance. Additional objectives were to eliminate the crowding and correct the maxillary dental midline.
Treatment alternatives
Based on the objectives, 2 treatment options were proposed. The first option consisted of increasing the arch length and opening a space for the missing central incisor along with restoration of the space with a bridge or an implant. The second option consisted of orthopedic and orthodontic treatment, including rapid palatal expansion to expand the maxilla in a transverse direction with reverse headgear to correct the maxillary retrognathia and anterior crossbite. The left lateral incisor could be substituted for the central incisor, and the left canine could be substituted for the lateral incisor; no bridge or implant would be necessary. This option seemed to be the most plausible.
The option of opening an edentulous space for a bridge would be difficult because of the inclination of the anterior teeth and the patient’s vertical skeletal pattern. Furthermore, it would most likely extend the treatment time. Considering all of these factors, we discussed the treatment options with the patient’s parents and then decided on the second option.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


