An open bite is a common malocclusion, and it is generally associated with several linked etiologic factors. When establishing the treatment plan, it is essential to consider every aspect of the various etiologic causes and their evolution; this will help to correct it. This article reports the case of a girl aged 10.7 years with a skeletal Class III malocclusion and an open bite. The treatment mechanics were based on compensatory dental changes performed to close the bite and correct the skeletal Class III malocclusion. The patient had a deep maxillary deficiency, and the lower facial third was severely enlarged. In this article, we aimed to describe a simple mechanical approach that will close the bite through changes in the occlusal plane (segmentation of arches). It is an extremely simple method that is easily tolerated by the patient. It not only closes the bite effectively but also helps to correct the unilateral or bilateral lack of occlusal interdigitation between the dental arches. A Class III patient with an anterior open bite is shown in this article to illustrate the effectiveness of these treatment mechanics.
An open bite is a deviation in the vertical relationship of the maxillary and mandibular arches, characterized by lack of contact between opposite dental segments. It can be associated with any type of malocclusion in the sagittal plane (Class I, Class II, or Class III).
A dental open bite is characterized by a reduction in the vertical growth of the dentoalveolar process in the affected area, generally associated with an oral habit (prolonged pacifier use, finger sucking, or altered swallowing habits) and a normal or favorable growth pattern. It is usually accompanied by incisor proclination and a reduced interincisal angle, and it generally responds to myofunctional treatment and mechanotherapy.
On the other hand, a skeletal open bite is due to a hyperdivergent phenotype with a vertical growth pattern that affects both the maxillary and mandibular bony bases. Because of its skeletal component, the orthodontic correction of a skeletal open bite is much more difficult, and there is no clear limit between what can be achieved by orthodontic compensation and what inevitably requires orthognathic surgery. Early treatment of the vertical dysplasia (during the deciduous or mixed dentition) might reduce the treatment needed in the permanent dentition when surgery is a valid option.
A logical question regarding this matter is where to place the limits of the dentoalveolar compensation. To answer this question, we report a patient with a Class III open-bite malocclusion and vertical skeletal dysplasia treated with camouflage orthodontic therapy.
Diagnosis and etiology
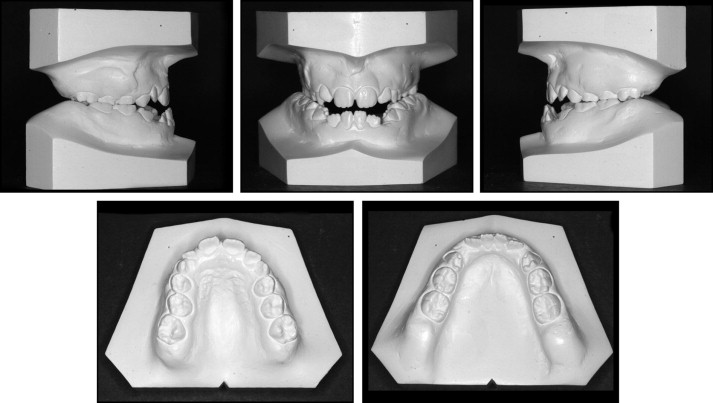
The patient was a girl aged 10.7 years with no relevant medical history or bone or dental pathology in her family history. The extraoral examination showed a distinct increase of the lower facial third, with slight mandibular asymmetry and midface deficiency along with a Class III profile ( Fig 1 ). The intraoral examination showed a Class III malocclusion with severe maxillary compression in all 3 planes that caused posterior and anterior crossbites (both with negative results). In the vertical plane, there were both anterior and lateral open bites.

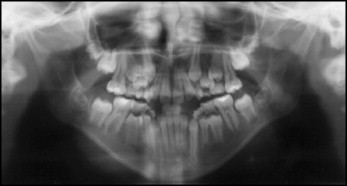
The mandibular dental cast ( Fig 2 ) showed that the deciduous canines were missing, and the incisors were retroclined. The mandibular arch-length discrepancy was −3.7 mm. In the maxillary arch ( Fig 3 ), a transverse deficiency and an arch length deficiency of −3 mm were noted. Moreover, a molar Class III relationship coexisted with the anterior and posterior crossbites and the previously mentioned open bite. The panoramic radiograph showed the lack of space for the permanent canines, and the condyles appeared thin and elongated, as normally seen in patients with vertical growth patterns ( Fig 4 ).
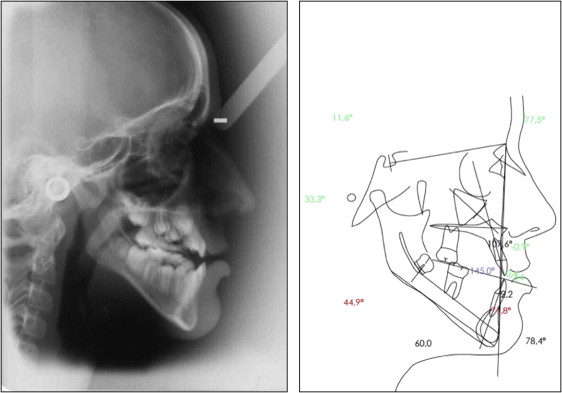
The cephalometric analysis was typical of a skeletal Class III pattern with a retruded maxilla and retroclined mandibular incisors (showing that the skeletal malocclusion was worse than it seemed because of the physiologic dentoalveolar compensation) in a hyperdivergent pattern with a significant vertical growth discrepancy.
Treatment objectives
The proposed treatment consisted of 2 phases: (1) correction of the crossbite and protraction of the maxilla with a facemask; and (2) (during the permanent dentition) leveling, alignment, and coordination of the dental arches, with bite closure and finishing of the occlusion. This treatment plan reflects the importance of treating the transverse and sagittal problems during the early stages and subsequently correcting the open bite through changes in the occlusal plane in the permanent dentition with a segmented arch approach.
The treatment plan involved 2 phases that took into account the eruption times and growth of the patient: (1) crossbite correction (maxillary disjunction with rapid palatal expansion) and traction with a facemask for dentoalveolar mobilization (phase 1); (2) a waiting period until dental eruption has been completed preceded by dental alignment; and (3) control of the open bite and the possibility of its closure (phase 2).
Complete correction of this type of malocclusion by providing only orthodontic treatment mechanics is especially difficult because of the underlying skeletal malrelationship. Therefore, the patient would need to undergo surgery if the response to dental compensation were not good enough. For this reason, in similar cases, orthodontic treatment seeks to improve some dental esthetic aspects, whereas the sagittal and transverse skeletal corrections are achieved through orthognathic surgery.
Class III patients with severe vertical problems are rather controversial, since all correction approaches, both sagittal and transversal, can severely worsen the vertical relationship. On the other hand, all vertical responses lead to improvements of sagittal Class III expression. In other words, it is difficult to improve vertical Class III problems while closing the bite. This depends on the magnitude of both problems and the way the mechanics are managed.
A bite-closure technique with segmented arches was used in this patient; it allowed us to obtain dentoalveolar closure thanks to a counterclockwise rotation of the occlusal plane without anterior vertical elastics, which could have increase the potential for relapse.
Treatment objectives
The proposed treatment consisted of 2 phases: (1) correction of the crossbite and protraction of the maxilla with a facemask; and (2) (during the permanent dentition) leveling, alignment, and coordination of the dental arches, with bite closure and finishing of the occlusion. This treatment plan reflects the importance of treating the transverse and sagittal problems during the early stages and subsequently correcting the open bite through changes in the occlusal plane in the permanent dentition with a segmented arch approach.
The treatment plan involved 2 phases that took into account the eruption times and growth of the patient: (1) crossbite correction (maxillary disjunction with rapid palatal expansion) and traction with a facemask for dentoalveolar mobilization (phase 1); (2) a waiting period until dental eruption has been completed preceded by dental alignment; and (3) control of the open bite and the possibility of its closure (phase 2).
Complete correction of this type of malocclusion by providing only orthodontic treatment mechanics is especially difficult because of the underlying skeletal malrelationship. Therefore, the patient would need to undergo surgery if the response to dental compensation were not good enough. For this reason, in similar cases, orthodontic treatment seeks to improve some dental esthetic aspects, whereas the sagittal and transverse skeletal corrections are achieved through orthognathic surgery.
Class III patients with severe vertical problems are rather controversial, since all correction approaches, both sagittal and transversal, can severely worsen the vertical relationship. On the other hand, all vertical responses lead to improvements of sagittal Class III expression. In other words, it is difficult to improve vertical Class III problems while closing the bite. This depends on the magnitude of both problems and the way the mechanics are managed.
A bite-closure technique with segmented arches was used in this patient; it allowed us to obtain dentoalveolar closure thanks to a counterclockwise rotation of the occlusal plane without anterior vertical elastics, which could have increase the potential for relapse.
Treatment alternatives
Patients with severe skeletal dysplasia require multiple treatments to solve their various problems. The treatment of patients with a Class III malocclusion is likely to require orthognathic surgery in adulthood. In other words, this approach will correct not only the dental problems, but also the facial and skeletal discrepancies. Treatment is not complete until the patient’s facial growth has ceased.
On the other hand, a first phase of treatment with initial control of the transverse and sagittal dimensions is considerably effective and useful for these patients. It improves the patient’s dentofacial appearance, and the remaining improvements can be achieved in the postgrowth stage through a surgical approach. Therefore, orthodontic treatment cannot be fully efficient but can sometimes help the patient, at least transversely, making the required surgical treatment less substantial.
A 2-phase treatment plan allows us to assess progress, and in patients whose response is positive, we can pursue a dentoalveolar correction. Orthodontic treatment will obviously not solve the skeletal problem, especially the vertical, since this can only be corrected by a surgical approach or by using temporary skeletal anchorage devices. They are a useful alternative when trying to reduce the anterior vertical dimension.
If there were a loss of the achieved objectives after growth and dental compensation are over, an orthognathic surgical treatment would be a valid option to resolve all problems and to obtain appropriate dentofacial harmony.
Treatment progress
Initially, a transpalatal arch was used during phase 1 to correct the mesial rotation and the torque of the molars. Placement of an expander was deferred because of the early stage of dental development. Meanwhile, anterior traction was performed with a facemask for a year.
Second, and as part of phase 1, rapid palatal expansion was achieved with a cemented hyrax appliance while continuing with the facemask to prevent sagittal relapse. Once the rapid palatal expansion was finished, a transpalatal arch was placed for retention. Maxillary and mandibular brackets were bonded ( Fig 5 ).
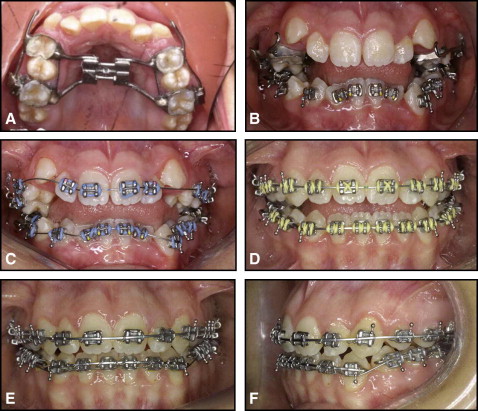
Closing the open bite with segmented arches involved a sequence that started with superelastic wires to align and level the dental arches. Once coordinated, the archwires were segmented in 3 sections: 2 sections including the molars and premolars, and a third section including all 6 anterior teeth. In the maxillary arch, a 0.021 × 0.028-in or a 0.019 × 0.025-in superelastic wire was used.
Similarly, in the mandibular arch, a 0.020 × 0.020-in superelastic archwire was used. At this point, triangular elastics were used to achieve bite closure in the premolar area and to modify the canting of the occlusal plane. Once these changes were accomplished, a thermoelastic 0.014-in overlay (piggyback) was placed to obtain an acceptable overbite. After closing the bite, the treatment was finished with a regular wire sequence ( Fig 5 ).
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


