This case report describes a new surgical orthodontic approach involving alveolar bone distraction osteogenesis for correction of an asymmetric maxillary dental arch. The treatment was combined with conventional orthognathic surgery to improve the mandibular lateral deviation. This new treatment strategy produced an ideal dental arch and a symmetric facial appearance efficiently and effectively.
An asymmetric dental arch associated with a skeletal problem often results in an asymmetric facial appearance. Improving the distorted facial appearance is one of the most critical objectives of orthognathic surgery. Several treatment techniques have been introduced for an asymmetric dental arch. A conventional nonsurgical orthodontic treatment gives an acceptable outcome if well-planned force mechanics are provided. However, they could induce root blunting, resorption, or fenestration during the treatment if the affected tooth-bone relationships are poor. Moreover, the treatment duration might be prolonged with traditional orthodontic treatment, because of those mechanical and physical complications. On the other hand, a surgical approach such as an osteotomy can correct skeletal problems immediately, although fixation of bone specimens sometime becomes difficult because it requires dexterous manipulation for fitting. Furthermore, even in a comparably simple procedure such as a corticotomy, sometimes the bone fixation can be challenging as well. Therefore, we suggest our new strategy, which overcomes the above-mentioned disadvantages, for treatment of an asymmetric dental arch.
Diagnosis and etiology
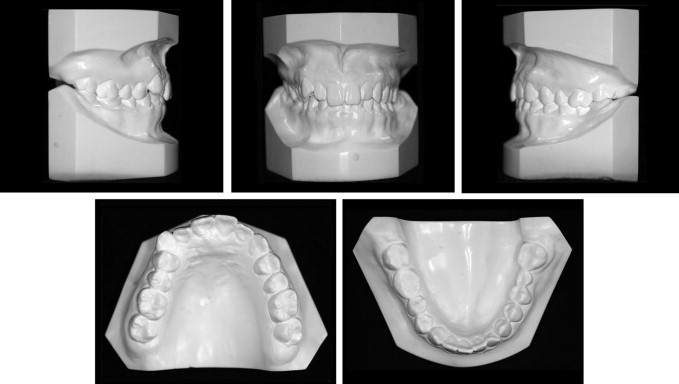
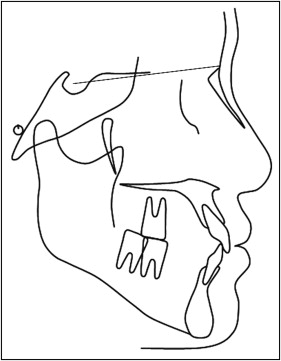
An 18-year-old Japanese woman was referred to the Department of Orthodontics at Nagasaki University Hospital in Japan for correction of her facial asymmetry. Her frontal facial appearance was not symmetric because of lateral deviation of the mandible, and the lateral profile was concave with normal facial height. The maxillary dental arch showed asymmetry because the right posterior teeth from the first premolar to the second molar were palatally inclined, but there was no posterior crossbite. The basal alveolar ridge on the maxillary right was collapsed to the palatal side as well. Overjet was 2.5 mm, and overbite was 2.0 mm. The mandibular midline was shifted 4 mm to the left. The molar relationship was Class I on the right and Class II on the left side. The canine relationships were Class III on the right and Class I on the left ( Figs 1 and 2 ). The panoramic radiograph showed that all permanent teeth were present except the first and third molars on the mandibular left side ( Fig 3 ). The cephalometric analysis showed that although the values of the SNA and SNB angles were within 1 SD, the ANB was −0.4°, showing mild mandibular prognathia. In addition, the facial angle, which represents the mandibular position, and the A-B plane, which represents the maxillomandibular relationship, were 88.3° (>1 SD) and −0.9 mm (>1 SD), respectively ( Table and Fig 4 ), showing a protruded mandible as well. The posteroanterior cephalometric radiograph detected no cant of the maxilla. Based on these findings, the patient was diagnosed with a skeletal Class III malocclusion with mandibular prognathism, facial asymmetry with mandibular deviation, and an asymmetric maxillary dental arch.


| Mean | SD | Patient | SD | |
|---|---|---|---|---|
| FH to SN plane (°) | 6.2 | 5.9 | 5.8 | |
| SNA (°) | 82.3 | 3.5 | 80.6 | |
| SNB (°) | 78.9 | 3.5 | 81 | |
| Facial angle (°) | 84.8 | 3.1 | 88.3 | ∗ |
| Gonial angle (°) | 131 | 5.6 | 121.6 | ∗ |
| Ramus angle (°) | 83 | 4.4 | 88.4 | ∗ |
| A-B plane (°) | −4.8 | 3.5 | −0.9 | ∗ |
| ANB (°) | 3.4 | 1.8 | −0.4 | ∗ |
| U1 to FH plane (°) | 111.1 | 5.5 | 117.1 | ∗ |
| L1 to mandibular plane (°) | 96.3 | 5.8 | 84.8 | ∗ |
Treatment objectives
The main objectives of this orthodontic treatment were to correct the facial and dental asymmetries and the maxillomandibular relationship. Therefore, the orthodontic treatment objectives were to (1) achieve a symmetric maxillary arch form, repositioning the retroclined maxillary right premolars and molars and the accompanying collapsed alveolar ridge by alveolar bone distraction osteogenesis; (2) establish a Class I mutually protected occlusion; and (3) improve the facial balance and deviation combined with orthognathic surgery.
Treatment objectives
The main objectives of this orthodontic treatment were to correct the facial and dental asymmetries and the maxillomandibular relationship. Therefore, the orthodontic treatment objectives were to (1) achieve a symmetric maxillary arch form, repositioning the retroclined maxillary right premolars and molars and the accompanying collapsed alveolar ridge by alveolar bone distraction osteogenesis; (2) establish a Class I mutually protected occlusion; and (3) improve the facial balance and deviation combined with orthognathic surgery.
Treatment alternatives
Intraoral vertical ramus osteotomy was selected to correct the lateral deviation of the mandible. Genioplasty was also required to correct the facial imbalance. Since there was no cant or rotation of the maxilla, a LeFort I osteotomy was not necessary. The following 3 treatment options for the asymmetric maxillary dental arch were considered for this patient.
- 1.
Conventional orthodontic treatment could be performed to obtain an ideal dental arch form. Although this would cause minimum physical strain on the patient, the possible risks such as root blunting, resorption, or fenestration would be induced by tooth rotation and uprighting during orthodontic treatment. In addition, for correction of the asymmetric facial appearance, an intraoral vertical ramus osteotomy and a genioplasty would be needed after the presurgical orthodontic treatment.
- 2.
All surgical procedures such as alveolar bone osteotomy from the right first premolar to second molar, plate fixations, and intraoral vertical ramus osteotomy with genioplasty could be performed at the same time. This alternative might be a standard procedure for treating such a patient; however, creating an ideal maxillary arch form to match the mandibular arch is difficult during the surgical procedure, because finding the best-fit positions of bone fragments and securing them for ideal relationships is complicated.
- 3.
First, corticotomy of buccal and palatal alveolar bones from the first premolar to the second molar on the right side of the maxilla could be performed with a 2-week time lag. Then the insecure maxillary right posterior ridge would be moved buccally by a distractor until an ideal arch shape is achieved. Finally, an intraoral vertical ramus osteotomy with a genioplasty would be performed to correct the facial imbalance. This alternative would require a longer treatment time than the second option. However, it had 2 advantages compared with the other treatment options: the orthodontist or surgeon can manage the amount of tooth-bone movement during the distraction until an ideal relationship is achieved; and root blunting, resorption, or fenestration can be prevented because the tooth-bone relationship is maintained during the distraction.
All 3 alternatives, and their risks and benefits, were explained to the patient. After the consultation, the patient, the orthodontist, and the oral surgeon chose the third strategy to eliminate concerns about prolonged treatment time and complicated surgical procedures as mentioned above.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


