Click on the DVD icon to watch the video
Aim
The aim of this chapter is to define intercuspal position (ICP) and its importance to both patients and dentists.
Outcomes
By the end of this chapter, the clinician should:
-
appreciate relevant aspects of the physiology and development of ICP
-
realise how ICP can be compromised, and the consequences of this
-
understand the dental and financial consequences of fitting a restoration that does not conform to ICP, and understand how to avoid this scenario.
Introduction 
For all of the complexity of the masticatory system, the most basic occlusal concept is very simple indeed: the top and bottom teeth need to meet together in a way that will allow food to be chewed and swallowed. ICP is the term we will use to describe the position in which the teeth are maximally meshed together. When a restoration is carved or shaped it is usually to conform to ICP. ICP is also the position on which orthodontic classifications are based. Clench your own back teeth together now and you have it (Fig 1-1). You can see how the teeth move into ICP on DVD animation A.
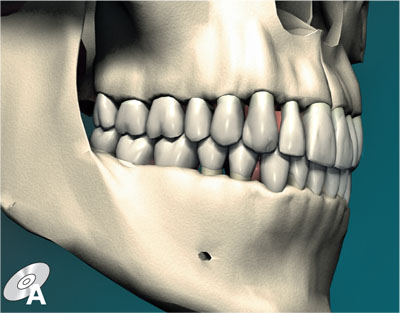
Fig 1-1 Teeth maximally meshed together in ICP.
Some dentists call this position “centric occlusion”, but we prefer to avoid this term as it means different things to different people. It can also cause confusion with the term “centric relation”, which is an important but very different concept (described in Chapter 3). Centric relation is determined by the temporomandibular joints (TMJs) but ICP is determined by the positions of the teeth, and because the two do not usually coincide the difference is important.
In this and the following chapters we will consider occlusally related damage. Damage from problems with ICP is often iatrogenic, the most familiar example being the damaging consequences of providing a high restoration.
Before looking at clinical problems and ICP, we will provide relevant background regarding its physiology and development. If you are interested in learning more, then the Further Reading section at the end of the chapter suggests appropriate material.
Physiology of ICP
Physiologically, ICP is the relationship of the mandible to the maxilla when the teeth reach the end of the chewing cycle. It is here, at the most closed position of the mandible, that the teeth apply maximum force. It is here that the teeth have closed through the food bolus to break up the food into smaller pieces, and it is also here that the mandible is stabilised, allowing swallowing to take place.
The bony architecture of the skull directs masticatory forces down the long axes of the teeth and into the robust base of the skull. This is a biomechanical triumph with various buttresses and arches transmitting crushing stresses without structural damage. Consider the forces involved in crunching through a nut kernel or breaking up tough fibres of meat – forces endured (incidentally) not only by the teeth, periodontium and bones, but also by restorations. Unlike in a simple nutcracker, however, there is a sensitive feedback system to regulate the amount of force applied to the teeth by the jaw muscles. Typically, forces will:
-
vary between 350 and 700 N (10 N approximates to 1 kg) for the maximum biting force
-
be about one-third of this during chewing
-
be several times higher in the molar than incisor regions.
The neuromuscular system which regulates these forces and jaw movements relies on proprioceptive input from the periodontal ligaments, the tooth pulps, the TMJs, muscles, tendons and ligaments. The periodontal ligament in particular is exquisitely sensitive, able to detect materials between the teeth down to 20 μm – half the thickness of a human hair – a fact worth remembering when placing and adjusting restorations. Also of direct clinical relevance is the potential for feedback from the pulp, predisposing root-treated teeth to higher forces as there is clearly no such feedback. This may partly explain the increased vulnerability of root-treated teeth to fracture.
Not only does the neuromuscular system regulate occlusal forces, it also programmes the muscular activity required to direct the teeth precisely into ICP without conscious effort. The frequent activity of swallowing constantly updates the neuromuscular system so that the muscles can position the mandibular teeth straight to ICP. This programming is impressive, but can make it difficult for the clinician to find and record other relationships of the mandible, such as centric relation. The muscles may need to be “deprogrammed”, as described in Section 8-4.
Although ICP is a fundamental concept in occlusion, paradoxically it is not a position held by the teeth for much of the time. Assuming we are in a reasonably relaxed state of mind, classical estimates are that the teeth only come together in ICP for 17.5 minutes a day, comprising approximately 1800 chewing strokes and 500 swallowing contacts. At other times the mandible is at rest, leaving a gap of a few millimetres between top and bottom teeth (Fig 1-2). It is perhaps not surprising then that the prolonged heavy contacts of parafunctional grinding and clenching are potentially damaging.

Fig 1-2 Most of the time the mandible is in the rest position with the teeth separated by 2–4 mm, termed “freeway space”.
Development of ICP
During occlusal development in childhood and adolescence, the moulding action of the tongue, cheeks and lips guides the erupting upper and lower teeth into position. In ICP, there appears to be a balance between the eruptive force of the teeth and the day-to-day masticatory forces. If a tooth erupts into a premature contact, it is subject to greater occlusal forces than the adjacent teeth, resulting in its orthodontic realignment. When a tooth is extracted, the balance is lost, accounting for the overeruption, tilting or rotational movements of adjacent and opposing teeth.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


