The term “fremitus” describes tooth mobility when occlusal contacts are performed. It may either be observed visually or felt through the examiner’s fingertips, or both. It may occur when the patient closes into the intercuspal or retruded positions, or during excursions of the mandible.
Occlusal factors may be important in the aetiology of increased mobility, but there are often other reasons. These are considered in the following section. Where the occlusion interacts with these factors, it may worsen or prevent resolution of the mobility. An increased mobility associated primarily to occlusal overload is relatively uncommon, but it can mystify the unwary dentist, particularly when it affects multiple teeth.
Non-occlusally Related Causes for Tooth Hypermobility
The commonest cause of increased tooth mobility is inflammatory periodontal disease. All clinicians are aware that teeth tighten after successful periodontal treatment, but increased mobility can persist after the inflammation has been eliminated. Characteristically, radiographs of affected teeth show reduced alveolar support, but a normal periodontal ligament space. This is simply an amplification of physiological mobility (Fig 5-1) because of long clinical crown height and short attachment. Despite the apparent increased mobility, such teeth do not require occlusal treatment if not subject to occlusal interference.
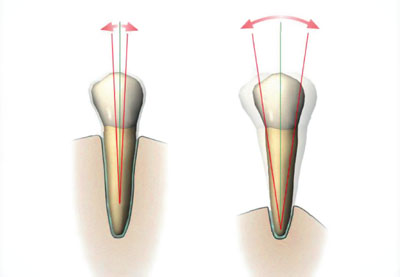
Fig 5-1 Although the tooth on the right is more mobile than the tooth on the left, the periodontal ligament is healthy and not widened. The increased mobility at the level of the occlusal plane is simply related to the longer clinical crown.
Only if the patient has discomfort from excessively hypermobile teeth during function, or if the mobility is increasing, might splinting be beneficial.
Other non-occlusal causes of increased mobility include:
-
root resorption
-
loss of periradicular bone support, for example due to periradicular inflammation or after apical surgery
-
recent trauma causing subluxation
-
fractured root
-
hormonal, occurring occasionally during pregnancy.
Occlusally Related Causes for Tooth Hypermobility
Habits such as bruxism can subject the teeth to loads which are higher and longer lasting than during normal function. This may, for poorly understood reasons, result in the periodontium adapting to the increased loads, rather than the neuromuscular system limiting load generation, as might be expected. Teeth with normal bone levels and normal attachment can still become hypermobile under such circumstances, with the response regarded as a physiological reaction to the mechanical insult. This is sometimes called “primary occlusal trauma”. Characteristically, the periodontal ligament becomes widened (Figs 5-2 and 5-3).
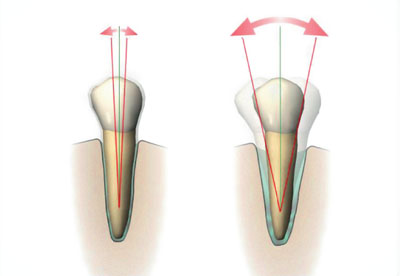
Fig 5-2 The tooth on the right shows the physiological response to a higher than normal occlusal force; its periodontal ligament has become widened (primary occlusal trauma).

Fig 5-3 A premolar with a widened periodontal ligament space. This is periodontal ligament widening, caused in this case by abnormal loading from a denture clasp.
The same physiological response of the periodontium can occur where there has been some change in the occlusal scheme, resulting in adversely changed loading, often non-axially directed. The increase in mobility can affect an individual tooth or a group of teeth. This might happen when a new restoration produces a premature occlusal contact or interference (direct occlusal trauma), or as a result of an occlusal interference somewhere else in the mouth causing a damaging deflection (indirect occlusal trauma). These problems are well illustrated in the DVD animations E, F and G. The same underlying mechanisms can sometimes explain migration of teeth and tooth positional relapse following orthodontic treatment (see the section Pathological Tooth Migration, below). 


Of course, teeth with a reduced but healthy periodontal support may undergo an increase in existing hypermobility if subjected to direct or indirect occlusal trauma. This is sometimes called “secondary occlusal trauma”. This terminology is not useful because the response to both primary and secondary occlusal trauma simply represents a normal physiological adaptation of the periodontium to increased occlusal loading.
A thorough clinical and radiographic examination will enable the cause of hypermobility to be identified. Increasing mobility is an important clinical symptom and sign to look out for. It can indicate an occlusal discrepancy which will benefit from correction.
In addition to conventional periodontal therapy, management of hypermobility caused by occlusal factors should be directed at:
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


