Chapter 65 The effect of polysomnography on pediatric adenotonsillectomy postoperative management
1 INTRODUCTION
Sleep disordered breathing (SDB) often presents in the pediatric population with loud snoring, respiratory pauses and mouth-breathing. For those with enlarged adenoids or tonsils, adenotonsillectomy can be curative. The decision for surgery is based upon the clinical history and physical examination. The polysomnogram is the gold standard for diagnosis of SDB, however, it is costly, time limiting and often not readily available and it is unclear which patient groups require or benefit from its use preoperatively.1,2 Several studies have identified populations at high risk for postoperative complications including children with craniofacial disorders, failure to thrive, neurological impairment, Down syndrome, obstructive sleep apnea and children age 3 or less.3–7 Because of the increased risk, preoperative polysomnography and postoperative overnight observation have been recommended for these patients to differentiate primary snoring from obstructive sleep apnea.8,9 In addition, several authors have concluded that polysomnographic results are predictive of postoperative complications and postoperative course.3–5,7 A recent retrospective study is summarized here which reviewed the postoperative course of children 3 years of age and younger and correlated these findings with the severity of obstruction as measured by preoperative polysomnogram.
4 RESULTS
The charts for 305 children age 3 years of age or younger were reviewed. Twenty-three children were excluded from the study for the following: incomplete chart (n=8), procedure miscoded (n=2), additional procedures performed (n=5), or procedure performed during period of acute illness (n=8). The remaining 282 sets of patient data were included in the statistical analysis. The average age was 30 months. Table 65.1 summarizes the age distribution. Upper airway obstruction was identified as the primary indication for surgery in 271 of the patients.
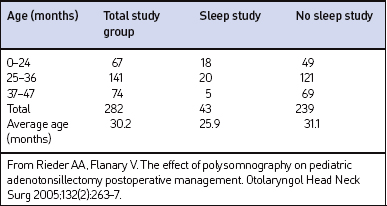
Sleep studies, including complete 16-channel (n=38), 4-channel (n=3), or hardcopy pulse oximetry (n=2), were performed preoperatively in 43 patients. The average age of patients that had a preoperative PSG was significantly younger at 25.9 months, compared to 31.1 months in the non-PSG group (P<0.0001). Twenty-seven patients were classified to have obstructive sleep apnea (OSA) (Res-piratory Disturbance Index [RDI] ranged from 1 to 52) and 11 were classified to have upper airway resistance syndrome (UARS). UARS was defined as abnormally increased upper airway resistance during sleep that led to increased respiratory effort and sleep fragmentation without defined apneic or hypopneic episodes or notable oxygen desaturations.10 Sleep studies without a calculated RDI or UARS were classified as normal, mildly abnormal, or significantly abnormal by the pulmonologist reading the study.
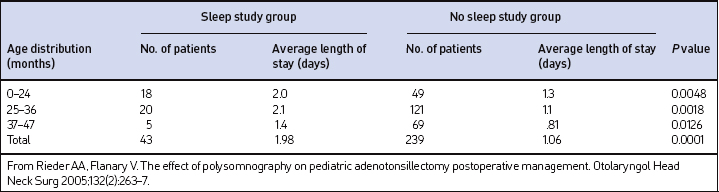
When the subjects were grouped using their RDI as a measure of OSA severity, there was no statistical difference between the average length of stay (LOS) for OSA patients. The average LOS for patients with UARS (2.2 days) was significantly longer when compared to the average LOS stay (1.57 days) for patients with OSA (P=0.0448). The average LOS, when calculated by age group in the non-PSG and PSG groups, was less in the non-PSG group at 1.06 days compared to 1.98 days in the PSG group (P<0.0001). The shortest average LOS occurred in the 37–47 month age distribution in both groups. The average LOS for both groups is listed in Table 65.2. The discharge criteria for patients typically required that the patients not require any supplemental oxygen and were able to maintain oxygen saturations above 90% without periods of sustained desaturation attributed to upper airway obstruction.
Complications were identified in 62 patients (21.9%). For this study, a complication was defined as any documented desaturation event (regardless of SaO2 nadir) or any other event/complication that required medical intervention or readmission, or prolonged the patient’s LOS. Complications occurred in 43 of 239 patients (17.9%) in the non-PSG group, and in 19 patients of 43 (44.2%) in the PSG group. Of those 62 patients, the most common complication identified was oxygen desaturation representing 65.1% of the total complications in the non-PSG group and 57.9% in the PSG group. Overall, desaturation events occurred in 13.8% (n=39) of the entire study population. Complications for each group are listed in Table 65.3.
| Group with sleep study (43) | Group without sleep study (239) | |
|---|---|---|
| Complication | No. of patients | No. of patients |
| Desaturation event | 11 (26%) | 28 (12%) |
| Poor oral intake | 6 (14%) | 10 (4%) |
| Pneumonia/atelectasis | 0 | 3 (1%) |
| Seizure | 0 | 1 (0.4%) |
| Bleeding | 1 (2%) | 1 (0.4%) |
| Death | 1 (2%) | 0 |
| Total no. of patientswith complications | 19 (44%) | 43 (18%) |
From Rieder AA, Flanary V. The effect of polysomnography on pediatric adenotonsillectomy postoperative management. Otolaryngol Head Neck Surg 2005;132(2):263–7.
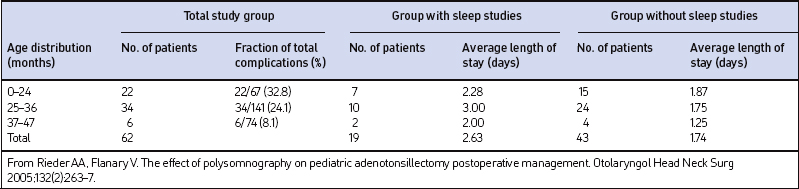
Table 65.4 lists the total complications and LOS by age group for the 62 patients with complications. The highest complication rate (32.8%) was found in children of 24 months and younger, while the lowest rate (8.1%) occurred in the group aged 37–47 months. There was no statistical difference in the mean age of the patients who had complications in the PSG group (26.5 months) compared to the non-PSG group (27.2 months) (P=0.7279). The average LOS for patients with complications in the non-PSG group was 1.74 days compared to 2.63 days in the PSG group. A trend toward a longer average LOS was identified in the PSG group but the difference did not reach statistical significance (P=0.0997).
< div class='tao-gold-member'>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


