Fig. 4.1
The balance between facial and tongue muscle forces. (a) The outer muscles, the orbicularis oris, buccinator, and superior constrictor muscles form a ring which acts to compress the palatal and mandibular arches with the teeth. (b) The tongue force acts to expand the dental arches and teeth. Whether the teeth and arches align is determined by the resultant of these forces
4.2 Aberrant Muscle Forces in Clefts of the Lip and Palate
A cleft of the lip and palate is the result of the failure of lip elements, and right and left palatal segments, to come together within the first 9 weeks of fetal life. The loss of muscular continuity of the orbicularis oris-buccinator-superior constrictor ring in complete unilateral and bilateral clefts changes the normal muscular force diagram. The aberrant muscular forces act to displace tissue masses. In complete clefts of the lip and palate, if the lateral palatal cleft segments are detached from the vomer, they will be pulled laterally by the external aberrant lip-cheek muscular forces, as well as spread apart by the tongue pushing into the cleft space (Fig. 4.2). Because clefts differ in their location and extent, lip and palate clefts can vary in the degree of geometric distortion, as well as in the size and shape of the cleft palatal segments.
Fig. 4.2
(a–d) Effects of complete clefts of the lip and palate at birth. In complete cleft lip and palate, with a separation in the orbicularis oris (a) buccinator (b) superior constrictor (c) muscle ring, the aberrant muscle forces plus the plunger action of the tongue causes the palatal segments to be pulled and pushed apart. (d) premaxillary vomerine suture. (a) In bilateral clefts of the lip and palate, the premaxilla may be laterally or ventrally flexed with the fulcrum at the premaxillary-vomerine suture. (b) Complete unilateral clefts of the lip and palate at birth. The cleft’s lesser segment and the premaxillary portion of the larger segment (d) are pulled outward. (c) Cleft of the lip and alveolus. The bony distortion is determined by the extent of alveolar involvement (Courtesy of J. D. Subtelny)
The muscular forces that act on the bony scaffolding of the palate and pharynx begin very early in intrauterine life; therefore, the palatal and facial configuration at birth has been formed over the major portion of the infant’s existence prior to birth.
In complete unilateral clefts of the lip and palate (CUCLP), the premaxillary portion of the noncleft segment is pulled anterolaterally. In addition to the lateral displacement of the lateral palatal segments, the premaxilla in the larger segment is carried forward in the facial skeleton. In complete bilateral cleft lip and palate (CBCLP), excessive growth in the premaxillary-vomerine suture is caused by increased tension at this site, precipitated by mechanical force stresses during periods of rapid growth (Berkowitz 1959; Pruzansky 1953, 1971; Friede 1973, 1977) (Fig. 4.3). This growth is continuous during early postnatal years and provides a fourth dimension to the deformity, which can alter the cleft palatal segments and their associated parts and either simplify or complicate treatment.
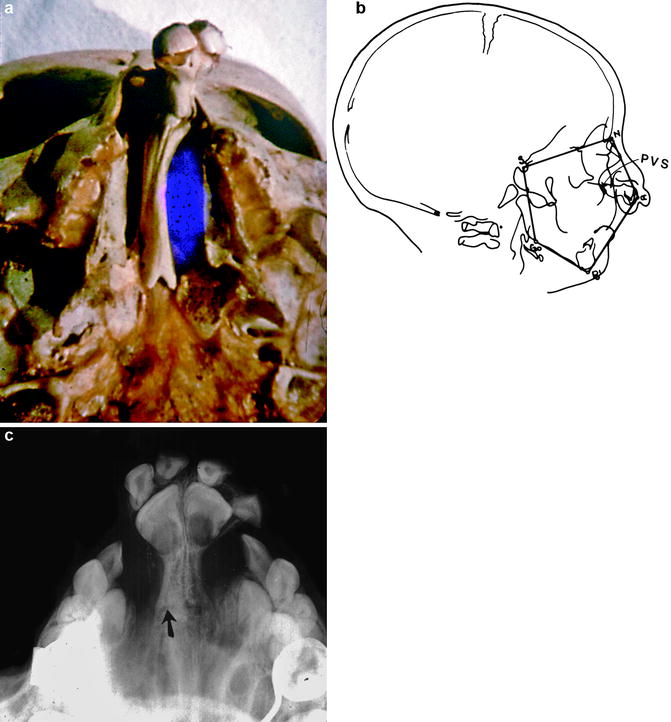
Fig. 4.3
(a–c) Skull with a bilateral cleft and palate. (a) The palatal segments have been overexpanded and the premaxilla protruded by the resultant aberrant muscle forces. The premaxillary-vomerine suture separates the premaxilla and the vomer and is a growth site. (b) Lateral cephalometric tracing at birth. Lines connecting various landmarks create a polygon depicting their geometric relationships. This tracing of a CBCLP at birth shows the degree of premaxillary protrusion. S Sella turcica, N Nasion, a Alpha (the anterior extent of the premaxilla), Po Pogonion, Gn Gnathion, Go Gonion, PVS Premaxillary-vomerine suture. (c) Occlusal radiograph of the premaxilla and vomer showing the premaxillary-vomerine suture (arrow)
If a soft tissue (mucous membrane, skin, and fibrous connective tissue), which collectively forms Simonart’s band, bridges the alveolar cleft, the attached palatal segments are limited in their degree of geometric displacement.
4.3 Categories of Clefts
Depending on the elemental characteristics of the embryology, anatomy, and physiology of the cleft defect, the varieties of clefts of the lip and palate may be tabulated into four general categories: (1) those involving the lip and alveolus, (2) those involving the lip and palate, (3) those in which the palate alone is affected, and (4) congenital insufficiency of the palate. The term “palate” will include both the hard palate and the velum, or soft palate (Fig. 4.4).
Fig. 4.4
(a–h) The anatomic classification system is based on the location, completeness, and extent of the cleft deformity. Because the lip, alveolus, and hard palate develop from different embryonic sources, any combination of clefting can exist. (a) Cleft of the lip and alveolus. Normal palate. (b) Isolated cleft of the hard and soft palate. Normal lip and alveolus. (c) Cleft of the soft palate and uvulae. (d) Cleft of the uvulae. (e) Complete unilateral cleft lip and palate. (f) Complete bilateral cleft of the lip and palate. (g) Incomplete bilateral cleft of the lip and palate. (h) Complete bilateral cleft of the lip and alveolus (Courtesy of Wolfe and Berkowitz (1989))
4.3.1 Clefts of the Lip (Figs. 4.5 and 4.6)

Fig. 4.5
(a) Complete unilateral cleft lip and palate. The distorted nostril is caused by the aberrant lip muscle forces. (b) Complete bilateral cleft lip and palate with a widely separated lateral palatal segment. The protruding premaxilla extends forward of the lateral palatal segments and is attached to the vomer. The prolabium (central portion of the lip) overlies the premaxilla

Fig. 4.6
(a, b) Incomplete clefts of the lip. (a) Unilateral and (b) bilateral
A cleft of the lip may be complete, extending from the vermilion border to the floor of the nose, or it may be incomplete. There are various degrees of incomplete lip clefts. Minimal defects involving only the vermilion border are observed. In others, the defect may extend to the nose as a submucous cleft in the muscle band, bridged only by mucous membrane, skin, and fibrous connective tissue. The nasal alar cartilage on the side of the cleft is displaced and flattened to a greater or lesser degree, depending on the extent and width of the cleft. The tip of the nose is deviated toward the noncleft side.
The cleft in the lip may be unilateral or bilateral, occurring on one or both sides, respectively. If bilateral, it may be symmetrical or asymmetrical, that is, it may or may not involve the lip equally on both sides (Fig. 4.5b). It should be noted that, in bilateral clefts, a median portion of the lip is isolated in the midline and remains attached to the premaxilla and to the columella. This portion of the lip contains the philtrum. In complete bilateral clefts of the lip, the premaxilla protrudes considerably forward of the facial profile (Fig. 4.5b). It is attached to a stalklike vomer and to the nasal septum. The columella appears to be deficient, and the alar cartilages are flattened on both sides. The effect on the facial profile is to accentuate further the protrusiveness of the premaxilla and the portion of the lip which is attached to the facial surface.
The more complete the defect in the lip, the greater the influence of the cleft on the alveolar process. Because of this constant relationship between the lip and alveolar process, it is not necessary to include the alveolar process as a separate entity in this description and classification. The maxillary alveolar processes arise from the mesoderm in the depths of a sulcus separating the lip and palate, while the tegmen oris gives rise only to the soft palate and the central part of the hard palate.
The relationship between the degree of the cleft’s effect on the alveolar process and defects in the deciduous and permanent dentition is interesting. The dental defect may be assessed in terms of the number of teeth, their shape, and structure as well as the position of the teeth in the dental arch. Irregularities in the alveolar process range from small dimples in association with minor clefts in the lip to actual grooves in the alveolar process to, in extreme cases of total clefts in the alveolar ridge, displacement of the premaxillary segment toward the noncleft side. Small dimples or grooves in the alveolar ridge tend to fill in as the jaw grows. However, the deciduous lateral incisor that erupts in this area may be T-shaped, or otherwise misshapen, and malpositioned in the line of occlusion. Further documentation and analysis of serial records should provide detailed information concerning the eruption of teeth adjacent to the cleft in the alveolar process.
4.3.2 Cleft Lip and Cleft Palate (Fig. 4.7)
Fig. 4.7
(a–e) Variations in the form, size, and extent of clefting in primary, secondary, and combined palatal clefts. Primary palatal clefts (with normal hard palate). Top row: (a) Normal lip. (b–g) The clefts may involve the lip only or may include the alveolus (tooth-bearing area) as well. The cleft can extend toward the nostril on one or both sides. Middle row: The cleft of the alveolus can extend to the incisal papilla on one or both sides to any degree. Bilateral alveolar clefts: (c) incomplete on both sides, (d) incomplete on one side and complete on the opposite side, and (e) complete on both sides. Secondary palatal clefts: (a) normal palate, (b) bifid uvula, (c) cleft of soft palate, (d) isolated cleft palate (moderate), and (e) isolated cleft palate (extensive). Combined palatal clefts. Unilateral: (a) Isolated CP with cleft lip and alveolus; (b
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


