Temporomandibular disorders (TMD) affect 5% to 12% of the United States population. This article discusses common conditions related to temporomandibular joints, including disc displacements, inflammatory disturbances, loose joint bodies, traumatic disturbances, and developmental conditions. Also addressed are the appropriate imaging modalities and diagnostic criteria for TMD.
Key points
- •
Temporomandibular disorder is the second most common chronic musculoskeletal condition after chronic low back pain. As pain-related TMD can affect an individual’s daily activities, psychosocial functioning, and quality of life, it is important to accurately diagnose these complex musculoskeletal disorders to provide the best clinical care.
- •
The new dual-axis diagnostic criteria for TMD offers an evidence-based assessment protocol for the clinician to use when screening patients for temporomandibular joint (TMJ) intra-articular disorders, but imaging is typically needed for a definite diagnosis.
- •
Both clinical history and examination, augmented as indicated with imaging, are needed to render proper TMJ intra-articular diagnoses. As several imaging modalities recommended in this article use ionizing radiation, careful clinical assessment with due consideration of the benefit to the patient must be carried out before ordering any imaging.
The temporomandibular joints (TMJs) play crucial roles in mastication and jaw mobility, and in verbal and emotional expression. Temporomandibular disorders (TMDs) include several disorders that can lead to orofacial pain symptoms. Box 1 presents a TMD taxonomic classification adopted from a publication by a panel of experts developing the diagnostic criteria for TMD (DC/TMD) for the most common TMDs, and the expanded TMD taxonomy for the more uncommon TMDs. It has been reported that about 5% to 12% of the United States population is affected by TMD, and the annual cost of managing TMD, excluding cost related to imaging, is about $4 billion. Plesh and colleagues reported that in the 2000 to 2005 US National Health Interview Survey (NHIS) that included a total of 189,977 people, 4.6% (n = 8964) people had experienced temporomandibular joint and muscle disorder (TMJD).
- I.
Temporomandibular disorders
- a.
Joint pain
- b.
Joint disorders
- i.
Disc disorders
- ii.
Hypomobility disorders other than disc disorders
- iii.
Hypermobility disorders
- i.
- c.
Joint diseases
- i.
Degenerative joint disease
- ii.
Systemic arthritides
- iii.
Condylysis/idiopathic condylar resorption
- iv.
Osteochondritis dissecans
- v.
Osteonecrosis
- vi.
Neoplasm
- vii.
Synovial chondromatosis
- i.
- d.
Fractures
- e.
Congenital/developmental disorders
- a.
- II.
Masticatory muscle disorders
- a.
Muscle pain
- i.
Myalgia
- ii.
Tendonitis
- iii.
Myositis
- iv.
Spasm
- i.
- b.
Contracture
- c.
Hypertrophy
- d.
Neoplasm
- e.
Movement disorders
- f.
Masticatory muscle pain attributed to systemic/central pain disorders
- a.
- III.
Headache
- a.
Headache attributed to TMD
- a.
- IV.
Associated structures
- a.
Coronoid hyperplasia
- a.
Progress in cross-sectional imaging using computed tomography (CT), MRI, and cone-beam CT (CBCT) has allowed better evaluation of the TMJ. Traditionally TMJ radiographic examinations included 2-dimensional images, such as transcranial, transmaxillary, and transpharyngeal projections, and submentovertex, lateral, and posteroanterior cephalometric radiographs. Conventional and panoramic tomography has also been used in TMD diagnosis but has limited use in assessing the TMJs.
The following sections provide a brief overview of the most common TMJ-related disorders and most appropriate imaging techniques. The latest recommendation from the panel of experts who developed the DC/TMD concluded that imaging should not be obtained routinely, but should be based on the clinical needs of the patient.
Disc displacement
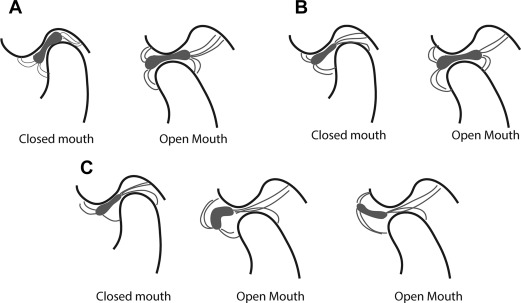
Disc displacement of the TMJ is a condition whereby the articular disc is displaced from its normal functional relationship with the condylar head and the articular fossa of the temporal bone ( Fig. 1 ). Disc displacement is considered to have 4 clinical stages.
- •
Stage I (disc displacement with reduction): the articular disc is displaced in closed-mouth position, and reduces to normal relationship, that is, the central narrow zone of the disc is in contact with the condylar head and articular eminence, in open-mouth position
- •
Stage II (disc displacement with reduction with intermittent locking): the disc is displaced in closed-mouth position, and intermittently locks in open-mouth position
- •
Stage III (disc displacement without reduction): the disc is displaced in closed-mouth position, and does not reduce to normal contact in open-mouth position (also referred to as closed lock)
- •
Stage IV (disc displacement without reduction): the disc is displaced and does not reduce, with perforation of the disc or posterior attachment tissues.
A commonly used classification of TMJ disc displacement, referred to as internal derangement, was described by Wilkes. This classification ( Table 1 ) described clinical and radiographic findings, the latter being based on MRI and tomography.
| Early stage (stage I) | Slight forward displacement and good anatomic contour of the disc. No osseous changes |
| Early/intermediate stage (stage II) | Slight forward displacement, and slight thickening of posterior edge or beginning anatomic deformity of disc. No osseous changes |
| Intermediate stage (stage III) | Anterior displacement with significant anatomic deformity/prolapse of disc (moderate to marked thickening of posterior edge). No osseous changes |
| Intermediate/late stage (stage IV) | Increase in severity over intermediate stage. Early to moderate degenerative osseous changes |
| Late stage (stage V) | Anterior disc displacement, nonreducing with perforation, gross anatomic deformity of the disc and hard tissues. Severe degenerative osseous changes |
Individuals with disc displacement can be asymptomatic. Persons who have disc displacement with reduction may have a normal range of jaw movement or limitations because of pain. Clinical examination may reveal joint sounds (eg, clicking and popping) during jaw movements. Individuals with disc displacement without reduction with limited opening may have deviation during opening toward the involved joint, and limited contralateral movements accompanied by pain and functional limitations, including compromised ability to eat.
Imaging
MRI of the TMJ in both closed and open positions is necessary for diagnosing stages of disc displacement ( Fig. 2 ). Other radiographic examinations, such as panoramic radiography or CT, are not useful in determining the location of the disc. In some individuals with a history of trauma, fluid effusion may be present. Effusion can be identified with T2-weighted MRI, whereby effusion has high signal intensity (see Fig. 2 E2, Table 2 ). The authors have updated the previous diagnostic criteria for disc displacement developed by their team (see Table 2 ).
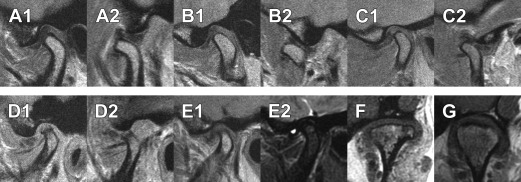
| Image Type | Mouth Position | Diagnosis | Posterior Band of the Disc | Intermediate Zone of the Disc |
|---|---|---|---|---|
| T1 or proton-density MRI, corrected sagittal view through the long axis of the condylar head | Closed mouth | Normal disc position | Relative to the superior aspect of the condyle, the border between the low signal of the disc and the high signal of the retrodiscal tissue is located between the 11:30 and 12:30 clock positions | Located between the anterior-superior aspect of the condyle and the posterior-inferior aspect of the articular eminence |
| Indeterminant disc position | Relative to the superior aspect of the condyle, the low signal of the disc and the high signal of the retrodiscal tissue is located anterior to the 11:30 clock position | The condyle contacts the intermediate zone located between the anterior-superior aspect of the condyle and the posterior-inferior aspect of the articular eminence | ||
| Relative to the superior aspect of the condyle, the low signal of the disc and the high signal of the retrodiscal tissue is located between the 11:30 and 12:30 clock positions | The intermediate zone of the disc is not in contact with the condyle | |||
| Displaced disc | Relative to the superior aspect of the condyle, the low signal of the disc and the high signal of the retrodiscal tissue is located anterior to the 11:30 clock position | The intermediate zone of the disc is located anterior to the condyle | ||
| Disc not visible | Neither signal intensity nor outlines make it possible to define a structure as the disc | |||
| Open mouth | Disc with reduction | Location of posterior band of the disc is not critical | The intermediate zone is located between the condyle and the articular eminence | |
| Disc without reduction | The intermediate zone is located anterior to the condylar head | |||
| T2 MRI, corrected sagittal view through the long axis of the condylar head | Closed mouth | Effusion present | A bright signal in either joint space that extends beyond the osseous contours of the fossa/articular eminence and/or condyle and has a convex configuration in the anterior or posterior recesses | |
| Effusion absent | No bright signal in either joint space, or a bright signal in either joint space that conforms to the contours of the disc, fossa/articular eminence, and/or condyle | |||
Disc displacement
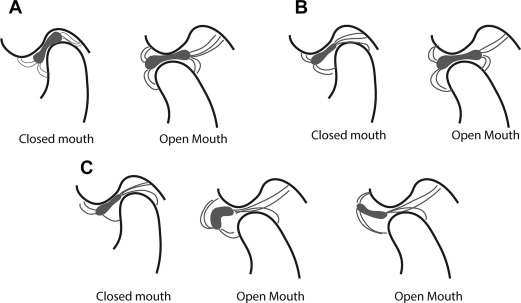
Disc displacement of the TMJ is a condition whereby the articular disc is displaced from its normal functional relationship with the condylar head and the articular fossa of the temporal bone ( Fig. 1 ). Disc displacement is considered to have 4 clinical stages.
- •
Stage I (disc displacement with reduction): the articular disc is displaced in closed-mouth position, and reduces to normal relationship, that is, the central narrow zone of the disc is in contact with the condylar head and articular eminence, in open-mouth position
- •
Stage II (disc displacement with reduction with intermittent locking): the disc is displaced in closed-mouth position, and intermittently locks in open-mouth position
- •
Stage III (disc displacement without reduction): the disc is displaced in closed-mouth position, and does not reduce to normal contact in open-mouth position (also referred to as closed lock)
- •
Stage IV (disc displacement without reduction): the disc is displaced and does not reduce, with perforation of the disc or posterior attachment tissues.
A commonly used classification of TMJ disc displacement, referred to as internal derangement, was described by Wilkes. This classification ( Table 1 ) described clinical and radiographic findings, the latter being based on MRI and tomography.
| Early stage (stage I) | Slight forward displacement and good anatomic contour of the disc. No osseous changes |
| Early/intermediate stage (stage II) | Slight forward displacement, and slight thickening of posterior edge or beginning anatomic deformity of disc. No osseous changes |
| Intermediate stage (stage III) | Anterior displacement with significant anatomic deformity/prolapse of disc (moderate to marked thickening of posterior edge). No osseous changes |
| Intermediate/late stage (stage IV) | Increase in severity over intermediate stage. Early to moderate degenerative osseous changes |
| Late stage (stage V) | Anterior disc displacement, nonreducing with perforation, gross anatomic deformity of the disc and hard tissues. Severe degenerative osseous changes |
Individuals with disc displacement can be asymptomatic. Persons who have disc displacement with reduction may have a normal range of jaw movement or limitations because of pain. Clinical examination may reveal joint sounds (eg, clicking and popping) during jaw movements. Individuals with disc displacement without reduction with limited opening may have deviation during opening toward the involved joint, and limited contralateral movements accompanied by pain and functional limitations, including compromised ability to eat.
Imaging
MRI of the TMJ in both closed and open positions is necessary for diagnosing stages of disc displacement ( Fig. 2 ). Other radiographic examinations, such as panoramic radiography or CT, are not useful in determining the location of the disc. In some individuals with a history of trauma, fluid effusion may be present. Effusion can be identified with T2-weighted MRI, whereby effusion has high signal intensity (see Fig. 2 E2, Table 2 ). The authors have updated the previous diagnostic criteria for disc displacement developed by their team (see Table 2 ).
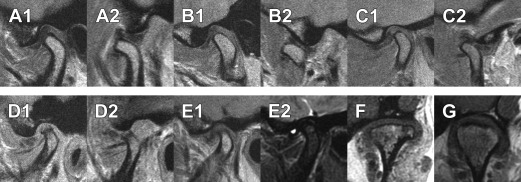
| Image Type | Mouth Position | Diagnosis | Posterior Band of the Disc | Intermediate Zone of the Disc |
|---|---|---|---|---|
| T1 or proton-density MRI, corrected sagittal view through the long axis of the condylar head | Closed mouth | Normal disc position | Relative to the superior aspect of the condyle, the border between the low signal of the disc and the high signal of the retrodiscal tissue is located between the 11:30 and 12:30 clock positions | Located between the anterior-superior aspect of the condyle and the posterior-inferior aspect of the articular eminence |
| Indeterminant disc position | Relative to the superior aspect of the condyle, the low signal of the disc and the high signal of the retrodiscal tissue is located anterior to the 11:30 clock position | The condyle contacts the intermediate zone located between the anterior-superior aspect of the condyle and the posterior-inferior aspect of the articular eminence | ||
| Relative to the superior aspect of the condyle, the low signal of the disc and the high signal of the retrodiscal tissue is located between the 11:30 and 12:30 clock positions | The intermediate zone of the disc is not in contact with the condyle | |||
| Displaced disc | Relative to the superior aspect of the condyle, the low signal of the disc and the high signal of the retrodiscal tissue is located anterior to the 11:30 clock position | The intermediate zone of the disc is located anterior to the condyle | ||
| Disc not visible | Neither signal intensity nor outlines make it possible to define a structure as the disc | |||
| Open mouth | Disc with reduction | Location of posterior band of the disc is not critical | The intermediate zone is located between the condyle and the articular eminence | |
| Disc without reduction | The intermediate zone is located anterior to the condylar head | |||
| T2 MRI, corrected sagittal view through the long axis of the condylar head | Closed mouth | Effusion present | A bright signal in either joint space that extends beyond the osseous contours of the fossa/articular eminence and/or condyle and has a convex configuration in the anterior or posterior recesses | |
| Effusion absent | No bright signal in either joint space, or a bright signal in either joint space that conforms to the contours of the disc, fossa/articular eminence, and/or condyle | |||
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


