Introduction
The purpose of this study was to examine the overall success of miniscrews inserted in the paramedian palatal region for support of various appliances during orthodontic treatment.
Methods
The patients received 1 or 2 miniscrews in the paramedian anterior palate of 8.0-mm length and 1.6-mm diameter placed during orthodontic treatment by the same experienced orthodontist.
Results
In total, 196 patients (121 girls, 75 boys; median age, 11.7; interquartile range, 3.7) who received 384 miniscrews were evaluated. Two hundred four miniscrews were used with rapid palatal expansion appliances, 136 with appliances for distalization of posterior teeth, and 44 with other appliances, such as transpalatal arches for tooth stabilization. The overall survival of the miniscrews was excellent (97.9%) in the cases examined. Cox regression analysis showed no difference in the overall survival rates of miniscrews loaded with different appliances for sex (hazard ratio, 0.95; 95% confidence interval, 0.71-1.27; P = 0.73) after adjusting for appliance and age.
Conclusions
This study shows that miniscrews placed in the paramedian anterior palate for supporting various orthodontic appliances have excellent survival.
Anchorage control is an important consideration during orthodontic treatment planning. Absolute anchorage seems to be accomplished by temporary orthodontic skeletal anchorage devices that include miniscrews, miniplates, and palatal implants. Incorporation of skeletal anchorage in current orthodontic practice requires that temporary anchorage devices allow for easy clinical application, immediate loading, easy removal, reasonable cost, and favorable primary stability and retention.
Although skeletal anchorage has been described as early as 1945, usage of miniscrews in orthodontics was incorporated in clinical practice only after 1997. Over the years, their use has become increasingly popular because they have adequately met the requirements of ease of clinical application and almost absolute anchorage. Recent evidence showed that skeletal and conventional anchorage systems as adjuncts to orthodontic treatment are perceived in a similar manner by patients.
Numerous articles, such as case reports and clinical trials, have been published documenting the applicability of various types of temporary anchorage devices in obtaining skeletal anchorage during orthodontic treatment, and various insertion sites have been proposed. A recent systematic review of bone anchorage systems for orthodontic application reported success ranges of 91.4% to 100.0% for miniplates, 74.0% to 93.3% for palatal implants, and 61% to 100% for miniscrews.
Depending on the orthodontic movement required, it could be in many cases advantageous if orthodontic skeletal anchorage devices are placed in other regions than in the interradicular alveolar bone. One such appropriate site is considered to be the hard palate: more specifically, the midsagittal plane or the paramedian region.
Until now, several studies have assessed the success of palatal implants for anchorage in orthodontic treatment. However, implants have 2 important disadvantages compared with miniscrews: they require, for osseointegration purposes, approximately a 3-month latency period before loading and consequently surgical intervention to remove them. Miniscrews have been placed in the midpalatal area with encouraging results, and recent studies have reported high success rates (90.8%-95.6%). Another option, especially for young patients whose palatal suture is not mature, is the placement of miniscrews in the paramedian palatal area, where the host hard-tissue parameters favor miniscrew placement.
To our knowledge, the survival of miniscrews placed in the paramedian palatal area has not been adequately investigated until now. Thus, the aim of this retrospective cohort study was to evaluate the survival of palatal miniscrews placed in paramedian regions and used for supporting various appliances during orthodontic treatment.
Material and methods
The sample was selected from a private orthodontic practice in Traben-Trarbach, Germany, and included all orthodontic patients treated with skeletal anchorage supported appliances placed in the palate. Patients received 1 or 2 miniscrews (Ortho Easy; Pforzheim, Forestadent, Germany) of 8.0-mm length and 1.6-mm diameter placed during orthodontic treatment by the same experienced orthodontist (B.L.). The miniscrews were inserted under superficial and subsequent local anesthesia in the anterior region of the palate, 3 to 6 mm paramedian to the suture and 6 to 9 mm distal to the incisive foramen. The insertion was performed with a surgical treatment unit with a maximum rotation rate of 60 rpm. In the same appointment, an impression was taken, and within 1 week an appliance was placed. The peri-implant soft tissues and the hygiene status were controlled in every appointment by visual inspection as a standard protocol. After insertion, all patients were told to minimize any possible contact of the miniscrews with their fingers or tongue. Furthermore, the patients were instructed to brush the miniscrews and abutments routinely once a day to prevent soft-tissue inflammation or overgrowth.
The orthodontic appliances supported by the miniscrews were of 3 main categories: rapid palatal expanion appliances, appliances for distalization of posterior teeth, and other appliances such as transpalatal arches for posterior tooth stabilization or segmented palatal arches for incisor stabilization ( Fig 1 ).

For each patient, the following data were collected: medical and dental histories, sex, age, date of miniscrew insertion, type of appliance, date of appliance insertion, and date of miniscrew and appliance removal, or date of failure of miniscrew or appliance. The primary outcome was miniscrew survival or failure.
Statistical analysis
Time to miniscrew success was explored with statistical methods for survival analysis, and miniscrew survival hazard ratios for sex adjusted for age and appliance were calculated with Cox proportional hazards regression modeling, accounting for clustering effects. For the calculation of the miniscrew and appliance survival period, the time from implant placement until appliance removal was used. In all cases, appliances were placed within 1 week after implant insertion, and no miniscrew failed before appliance placement. The proportional hazard assumptions were assessed using log-log plots, comparing fitted and predicted Kaplan-Meier plots, and on the basis of Schoenfeld residuals. All analyses were conducted with the STATA statistical package (version 12.1; StataCorp, College Station, Tex).
Results
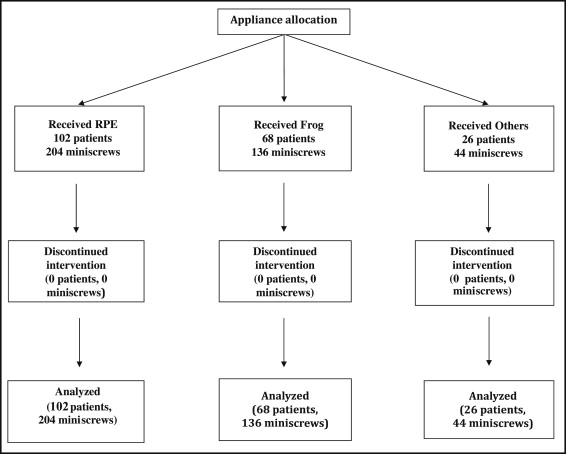
In total, 384 miniscrews that supported 196 appliances were inserted for orthodontic anchorage purposes in the paramedian anterior palate of 196 patients in a 5-year period (June 2006-May 2011). Patient flow is shown in Figure 2 , and their demographic and clinical characteristics are summarized in Table I .
| Total n = 196 | RPE appliance n = 102 | Distalization appliance n = 68 | Other appliance n = 26 | |
|---|---|---|---|---|
| Sex (%) | ||||
| Female | 60.8 | 60.8 | 60.3 | 65.9 |
| Male | 39.2 | 39.2 | 39.7 | 34.1 |
| Age (y), median (IQR) | 11.7 (10.1-13.8) | 12.0 (9.2-14.0) | 10.9 (10.2-12.6) | 14.9 (12.2-30.3) |
Of the entire sample, only 8 patients received 1 miniscrew on the right side of the palate, and all were in the “other appliances” group. Single miniscrews were used only for indirect anchorage. The remaining 188 patients received 2 miniscrews each, one at the right and the other at the left side of the palate, for appliance support. At the end of the observation period, 13 patients (25 miniscrews: 12 with 2 miniscrews, and 1 with 1 miniscrew) were still in treatment.
The survival of the miniscrews was excellent in all cases examined, as shown in Table II . Of 384 miniscrews, only 8 failed; 2 were in the same patient. Of the failed miniscrews, one that supported a rapid palatal expansion appliance broke after 2.3 months of use, and the remaining 7 were removed because of extensive mobility.
| Overall 384 miniscrews (%) | RPE appliance 204 miniscrews (%) | Distalization appliance 136 miniscrews (%) | Other appliances 44 miniscrews (%) | |
|---|---|---|---|---|
| Sex | ||||
| Female | 3/235 (99.1) | 2/124 (98.4) | 0/82 (100.0) | 1/29 (96.6) |
| Male | 5/149 (96.6) | 2/80 (97.5) | 3/54 (94.4) | 0/15 (100.0) |
| Overall | 8/384 (97.9) | 4/204 (98.0) | 3/136 (97.8) | 1/44 (97.7) |
| Age group (y) | ||||
| <10 | 3/95 (96.8) | 3/62 (95.2) | 0/30 (100.0) | 0/3 (100.0) |
| 10-11.6 | 2/96 (97.9) | 0/30 (100.0) | 2/62 (96.8) | 0/4 (100.0) |
| 11.7-13.7 | 1/96 (99.0) | 0/50 (100.0) | 1/34 (97.1) | 0/12 (100.0) |
| >13.8 | 2/97 (97.9) | 1/62 (98.4) | 0/10 (100.0) | 1/25 (96.0) |
| 8/384 (97.9) | 4/204 (98.0) | 3/136 (97.8) | 1/44 (97.7) |
Failures were evenly distributed in the 5-year interval when the appliances were used; thus, the potential influence of experience with appliances on miniscrew survival was not evident.
Table III shows the number of successful miniscrews, medians, and range of months of follow-up overall, and by sex and type of appliance.
| Total (n) | Successful miniscrews (n) | Median follow-up time (mo) | Range of follow-up time (mo) | |
|---|---|---|---|---|
| Female | 235 | 232 | 5.5 | 1.1-23.8 |
| Male | 149 | 144 | 5.6 | 0.4-17.5 |
| RPE appliance | 204 | 200 | 5.1 | 1.1-17.4 |
| Distalization appliance | 136 | 133 | 6.3 | 1.6-23.8 |
| Other appliances | 44 | 43 | 6.8 | 0.4-21.6 |
| All | 384 | 376 | 5.5 | 0.4-23.8 |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


