Chapter 56 Speech-ready, long-termtube-free tracheostomy for obstructive sleep apnea
1 INTRODUCTION
Obstructive sleep apnea (OSA) is caused by obstacles to the free flow of air through the upper airway from the lips or nasal tip to the larynx and therefore is within the otolaryngologist’s sphere of responsibility. Management can involve weight loss, treatment of nasal obstruction, surgery of the pharynx, or the use of various ventilatory assist devices such as continuous positive airway pressure (CPAP). This condition has serious health risks and consequences and should be thoroughly researched and investigated to be treated effectively. Furthermore, it is often multifactorial, requiring a multidisciplinary approach to identify the etiology and optimal treatment for each patient.
1.1 SEMANTIC CLARIFICATION
Historically, the documented performance of tracheo-tomy (semantically misrepresented as tracheostomy) for ‘Pickwickian syndrome’ was first described in 1969.1 Since then various modifications of the procedure have evolved into the ‘gold standard’ for management of OSA because, when successful, it bypasses upper airway obstruction in 100% of the cases in which it is used.2 Unfortunately, as mentioned above, patients with OSA are often difficultcandidates for performance and maintenance of routine tube-dependent tracheotomy; their unfavorable anatomy may be compounded by obesity, diabetes, infection and cardiopulmonary comorbidity. With each negative experience, lessons were learned that led to modifications of tracheotomy as it related to the treatment of OSA. Through this process, tracheotomy evolved into increasingly refined techniques such as tube-dependent tracheostomy and subsequently into the tube-free tracheostomy which has been researched, promoted and formulated by the authors. Further classification of these terms is provided below.
3 TRACHEOTOMY AND TUBE-DEPENDENTTRACHEOSTOMY
‘Standard tracheotomy’ might be performed in situations in which the duration of cannulation is not expected to exceed several days. These tracheotomies might be performed in OSA if they are used to temporarily securethe airway while other upper airway surgery performed. Even then, the technique may require modifications such as lipectomy or resort to specially designed and constructed tubes in order to be safe and effective. Once postoperative edema is resolved and the risk of perioperativehemorrhage and any other problems have been overcome, the tracheotomy tube may be withdrawn and the tracheo-tomy site allowed to heal by secondary intent. If prolonged cannulation is expected, such ‘standard tracheotomy’ (even when modified) is not the procedure of choice. Patientswith severe obstructive sleep apnea are prone to develop more serious complications as they often have short, thick necks and high incidence of anatomic deformations. Chondritis, granulation tissue, infection, and stenosis make long-term maintenance of a ‘temporary standard tracheo-tomy’ undesirable.2
Techniques for ‘permanent’ tracheostomy were developed in order to minimize these complications whenever cannulation is expected to be prolonged.3 Among the several indications for establishment of a ‘permanent’ skin-lined tracheostoma are severe laryngeal or laryngotracheal stenosis, bilateral vocal cord fixation (conditions that may cause OSA in and of themselves), neurologic conditions such as myasthenia gravis and amyotrophic lateral sclerosis, and, of course, severe OSA. The first report of permanent tracheostomy for the management of pulmonary disease was by Penta and Mayer4 in 1960; the technique was subsequently popularized for OSA by Fee and Ward5 in 1977. These techniques aim to decrease the length of the tracheocutaneous tract and bring the margins of the tracheal fenestration into direct contact and continuity with the cervical skin. Shortening the skin-to-trachea tract limits granulation tissue within the wound bed, promotes primary healing of the mucocutaneous junction, inhibits stomal stenosis, and aims to limit other complications associated with prolonged tracheotomy.
There are several techniques for creating a ‘permanent’ tracheostoma depending upon the degree of continuity established between the trachea and the cervical skin. One early method for creation of a permanent tracheostomy was the Bjork flap, in which an inferiorly based tracheal flap (generally created from the anterior portion of the second or third tracheal ring) is sutured to the inferior skin margin.6 Use of this flap relative to standard tracheotomy reduced rates of accidental decannulation and facilitated re-insertion of a displaced tracheotomy tube.7 Later methods for tracheostomy attempted to further improve the primary attachments between the trachea and the skin. An example is the ‘H-flap’ technique described by Mickelson.2 By mobilizing both cervical skin and tracheal flaps, a fully circumferential stoma is created through this technique.
4 REVIEW OF THE LITERATURE ON THEEFFICACY OF TRACHEOTOMY ANDTRACHEOSTOMY IN OSA
Once successfully performed, tracheotomy or tracheo-stomy should provide secure and complete bypass of any ventilatory obstruction proximal to the tracheotomy’s point of entry into the trachea. This achievement is unmatched by any other form of therapy for OSA. In one study, for instance, tracheostomy successfully relieved OSA in 24 patients; 22 of these patients had already failed other treatment modalities.8 Nor does the efficacy of tracheostomy fade with time, provided that local tracheal complications are avoided. A retrospective review of 79 patients with tracheostomies for OSA reveals that, even with a mean follow-up of over 8 years, tracheostomy eliminated the obstructive component in OSA in all cases.9 Long-term follow-up suggests that tracheostomy improves parameters such as Apnea/Hypopnea Index, snoring, and excessive somnolence with efficacy unmatched by any other therapy.10
Another benefit of tracheostomy is the immediacy with which it cures OSA. Obstruction is relieved soon after the tracheostomy is established. Polysomnographic measures of sleep architecture reveal that delta-wave and REM sleep are greatly increased soon after tracheotomy, in a ‘rebound’ phenomenon in which the body attempts to replenish those stages of deep sleep lost to apneic episodes.2 Within 1 month following tracheostomy, normal sleep architecture is returned; within weeks after tracheostomy, patients experience resolution of daytime sleepiness and snoring.11 In association with these improved sleep parameters, Guilleminault et al. also found that tracheostomy resolved the personality changes, erratic behavior, enuresis, morning headache, sleepwalking, and other symptoms related to OSA.12
Other studies demonstrate the effectiveness of tracheo-stomy in reducing the mortality associated with OSA. He et al. found that in patients with apnea indices >20, the 38% 8-year mortality of untreated patients was reduced to 0% in 33 patients with tracheostomy.13 Partinen et al. report similar findings in their cohort of 198 patients, 71 treated with tracheostomy and 127 treated conservatively with weight loss.14 All deaths at 5 years were in the weight loss group with a 5-year mortality rate of 11% as compared to 0% for tracheostomy. These differences in mortality are even more remarkable given that the tracheostomy group had, on average, higher apnea and body mass indices than the comparable weight loss group.
One early study on tracheostomy and hemodynamic changes in OSA was published by Motta et al. in 1978.11 Comparing patients with OSA before and after tracheo-stomy, these investigators found that during sleep, mean pulmonary and femoral artery pressures were significantly reduced following tracheostomy, while arterial oxygen levels were increased. Although the underlying mechanisms of increased cardiovascular morbidity and mortality are not entirely understood, one postulated etiology is that repeated hypoxic events in OSA initiate oxidative stress, cause endothelial cell dysfunction, and exacerbate atherogenic injury.15
Unfortunately, there are some limits to the effectiveness of tracheostomy for treatment of sleep apnea. First, tracheostomy can successfully treat only obstructive sleep apnea; central apnea may continue to be a problem for these patients. Indeed, one case report even describes the obstructive apneas corrected by tracheostomy being replaced by central events of similar duration and severity.16 Second, tube-dependent tracheostomy can only provide effective bypass of upper airway obstruction as long as the tube remains patent. In a patient with a large body habitus, excess soft tissue or skin folds over the chest and under the chin may actually obstruct the tube’s proximal end. It is for that reason that some authors recommend specially designed tubes in addition to adequate lipectomy in combination with tracheostomy for obese patients.17 Misalignment between the tube and the trachea may result in impaction of the tube’s caudal end against the tracheal wall, causing local ridge formation or stenosis, both of which may be compounded by traumatic suctioning. Unfortunately, patients with OSA compounded by cardiopulmonary decompensation may be more prone to complications including infections and even persistent apnea following tracheostomy (from central events, stenosis or tube obstruction) than patients with ‘uncomplicated’ OSA.18
5 COMPLICATIONS OF TUBE-DEPENDENTTECHNIQUES (TRACHEOTOMY OR TUBE-DEPENDENT TRACHEOSTOMY)
The complications of tube-dependent tracheotomy/tracheo-stomy can generally be divided into short-term and long-term categories. Short-term complications include possible intraoperative consequences such as damage to the great vessels, injury of the tracheo-esophageal party wall, pneumothorax, and pneumomediastinum. Early postoperative consequences of tracheotomy such as tube obstruction, tube displacement, and infection can also be considered short-term complications. Among the long-term complications are such problems as deep tissue infection, granulation tissue and laryngeal and/or tracheal stenosis at the stomal level or at the caudal end of the tube with predisposition to tracheo–innominate artery fistula. In addition to these physical complications, the often persistent morbidity associated with tube-dependent tracheostomy may have emotional consequences (such as depression) as well, for both the patient and the patient’s family.12,19
Several studies have documented the incidence of short-term complications following tracheotomy/tracheostomy for OSA. Thatcher and Maisel’s review of 79 patients counts four instances of peristomal wound infection, four instances of skin flap necrosis, and one fatal episode of cardiac arrest among early complications.9 Harmon et al. report a 15% incidence of peristomal infection following tracheostomy for OSA,20 while Guilleminault et al. suggest that the incidence of low-grade infection causing peristomal granulation may be closer to 42%.12 This same group also reports that a similar percentage (42%) of patients experienced early problems with poorly fitted tracheotomy tubes, such that the tube would become obstructed when the patient’s head was flexed, hyperextended or turned to the side.
Postobstructive pulmonary edema has been commonly reported following relief of short-term upper airway obstruction, such as that found with postoperative laryngospasm.21 However, postobstructive pulmonary edema has also been described as a consequence of OSA, perhaps secondary to effects of OSA on the heart and pulmonary vasculature.22 Given that tracheostomy for severe OSA provides immediate relief of prolonged upper airway obstruction, it should not be surprising that postobstructive pulmonary edema has been described in this setting as well. Comparing 45 OSA patients to 25 non-OSA patients, Burke et al. found an incidence of pulmonary edema of 67% in the OSA group following tracheotomy as compared to a control group incidence of 20%.23 While most OSA patients with post-tracheotomy pulmonary edema were graded as ‘mild’, 8/30 patients with pulmonary edema were graded as ‘moderate’ or ‘severe’ and two patients (7% of the overall OSA group) died of complications related to cor pulmonale in the post-tracheotomy period.
Among long-term complications of tracheostomy, tracheo–innominate artery fistula is the most feared. Though rare (only one of 79 patients in Thatcher and Maisel’s study9), it carries a mortality rate of 73%. One controllable factor which might predispose towards fistula is a ‘too low’ tracheotomy, and for this reason, tracheotomy is rarely performed beneath the third tracheal ring. Unfortunately, emphysematous, barrel-chested, or overweight OSA patients may have a high innominate artery, mandating modifications in the surgical procedure that may promote additional damage, to the larynx in particular.
A much more common long-term complication of tracheostomy is progressive, tube-related deformation of the trachea itself, including the development of laryngotracheal stenosis. Estimates of long-term tracheal damage following tracheostomy for OSA vary and depend on the surgical technique and endpoint used in each study. For instance, Conway et al.19 reported on eight patients with standard tracheotomy and found that seven (87.5%) experienced tracheal granuloma or stomal stenosis. Among eight patients (five revision, three primary) with skin-lined permanent tracheostomy, the incidence of tracheal complications decreased to 25%. Thatcher and Maisel do not record the overall proportion of patients who developed granulation tissue, but document that eight of 79 (10%) of their cohort needed to return to the operating room for management of this problem.9
Such retrospective studies might underestimate the degree of structural laryngotracheal deformities, infections, chondritis, granulation tissue and stenosis compared to prospective studies. Law et al. review several studies and find that retrospective reviews report obstructive tracheal lesions at rates of 1–11%, while prospective studies find obstructive lesions in 20–64% of patients with long-term tracheostomies.24 Their own study of 81 patients with long-term tracheotomy (mean duration 4.9 months) utilizing fiberoptic bronchoscopy prior to decannulation discovered obstructive lesions in 54 patients (67%). Of these 54 patients with tracheal obstruction secondary to prolonged tube-dependent tracheotomy, almost half (23 of 54, 43%) had more than one type of obstructing lesion. All of the lesions were located above the level of the stoma, and included 45 obstructing tracheal granulomas (all from the anterior tracheal wall), 19 patients with tracheomalacia, and 10 episodes of tracheal stenosis.
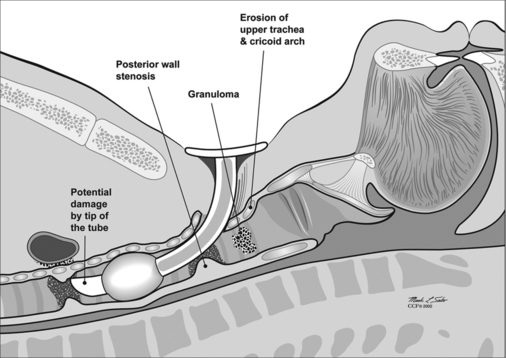
Unfortunately, damage to the trachea and larynx above the level of the stoma is too commonly an unavoidable consequence of prolonged cannulation with a curved tracheotomy tube. The introduction of a mismatched curved foreign body (the routinely used tracheotomy tube) into an otherwise straight airway displaces the suprastomal portion of the anterior tracheal wall inwards (Fig. 56.1). This pathologic buckling of the trachea is an unrelenting dynamic process perpetuated by the movements of the tube relative to the trachea during coughing, breathing, swallowing, and manipulation of the tube for cleaning. In this fashion, progressive deformation of the trachea can erode the anterior superior tracheal wall and lead to suprastomal inflammation, infection, granulation, perichondritis, chondritis and eventually necrosis, potentially extending to the cricoid arch and conus elasticus. When the tube is withdrawn, various degrees of tracheomalacia and tracheal stenosis may occur. Variations of standard tracheotomy tubes (i.e. tubes that are narrower, smoother, softer, more flexible, shorter, etc.) can help reduce but cannot eliminate the laryngotracheal morbidity associated with prolonged cannulation.25
< div class='tao-gold-member'>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


