Chapter 25 Snare uvulectomy for upper airway resistance
1 INTRODUCTION
The upper airway resistance syndrome (UARS) defines a group of patients with clinical signs and symptoms of excessive daytime somnolence in absence of obstructive sleep apnea. Often these patients complain of snoring. These patients have increased upper airway resistance which is characterized by partial collapse of the airway resulting in increased resistance to airflow. Physical findings often include excessive palatal tissue and narrowing of the oropharynx and hypopharynx. The increased respiratory effort required results in multiple sleep fragmentations as measured by very short alpha EEG arousals.1 In some cases, snoring may not be a feature of UARS. The resistance to airflow is typically subtle and does not result in apneic or hypopneic events; therefore a normal respiratory index is recorded. However, it does result in increasingly negative intrathoracic pressure during inspiration, which can be measured using an esophageal manometer as an adjunct to a polysomnogram. Therefore, diagnosis rests on symptoms of excessive daytime somnolence coupled with polysomnographic documentation of >10 EEG arousals per hour of sleep. These EEG arousals are correlated with episodes of reduced intrathoracic pressure, as noted on esophageal manometry. The esophageal pressure monitoring is an indirect measurement of upper airway collapse and when the esophageal pressure readings exceed −10 cm of water the work of breathing is increased and polysomnogram with electroencephalogram monitoring will pick up these alpha arousals.2 The frequency of alpha arousals during sleep is thought to be the major contributing factor for daytime somnolence.
2 PATIENT SELECTION
Patients with symptoms of UARS and normal respiratory disturbance indices should be considered for snare uvulectomy if the palate has already been treated or excluded as part of the pathology of sleep disordered breathing.2 Patients with an elongated uvula which touches the base of the tongue or those with an edematous mucosal uvula are considered to have uvular hypertrophy and will have the most significant tissue volume reduction. The uvula is targeted in other minimally invasive surgery to treat UARS which has included laser-assisted uvulopalatoplasty, bovie uvulectomy, injection snoreplasty, and radiofrequency submucosal needle therapy. The purpose of this chapter will be to describe the current technique of palatal volume reduction through the means of uvulectomy with a hot snare. It has the advantage of limiting thermal mucosal injury because the precision of the wire and the central squeeze makes for a clean amputation. It should be noted that the procedure itself is not a new one; indeed it dates back to Greek physicians in the Byzantium era.3 The modern form of the procedure is performed strictly in a clinical setting with local anesthesia. In cases where both palatal and/or uvulectomy do not improve the UARS, procedures related to the tongue base or medical treatment with CPAP are alternatives.
3 OUTLINE OF THE PROCEDURE
The anesthetic technique is similar to that of preparation for laser uvulopalatoplasty. The oropharynx is sprayed with 20% benzocaine (Hurricane Spray, Beutlich, Waukegan, IL) followed by injection with 1.5 ml of equal mixture of 1% lidocaine with 1:100,000 epinephrine (Abbott, North Chicago, IL) and 0.25% bupivacaine through a one and a quarter inch 27-gauge needle attached to a 3 ml syringe (Figs 25.1 and 25.2).
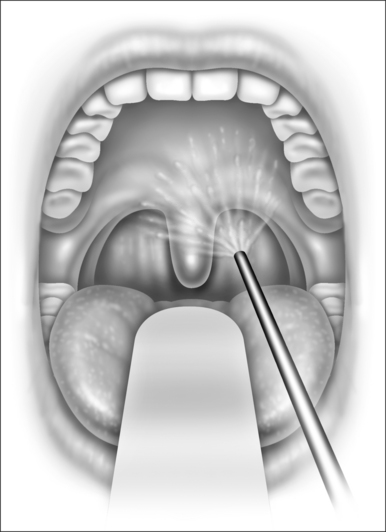
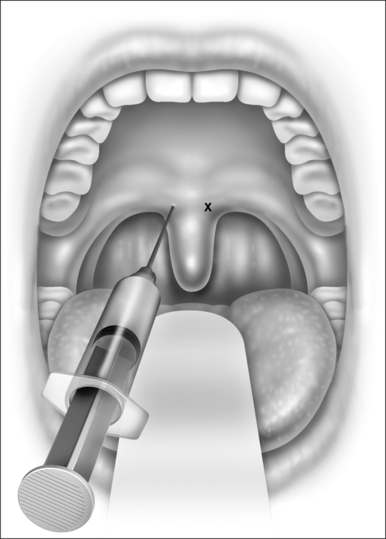
Fig. 25.2 Injection of local anesthetic at the neck of the uvula. Injection is within the muscle layer.
< div class='tao-gold-member'>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


