The purpose of this article is to present a simple method for determining the optimal sizes of anterior teeth. This is needed because of the frequency of anomalous and missing maxillary lateral incisors. In addition to anomalous and missing incisors, other factors that create challenges for the dentist and orthodontist when designing an esthetic and occlusally sound dentition are attrition, trauma, transposition, erosion, and caries. Optimal esthetics and occlusion require correctly sized teeth in proportion to themselves and the other teeth. Orthodontics, in partnership with restorative dentistry, allows doctors to accomplish the objectives of ideal occlusion and enhanced esthetics. Data compiled from previously published research enabled us to create simple formulae to determine optimal tooth sizes, an esthetic guide worksheet to use with collaborating dentists, and a sample written communication to accompany the completed esthetic guide worksheet. The method for establishing optimal tooth sizes is presented in a manner that allows easy memorization of the formulae and determination of the best dimensions for teeth without the use of a calculator.
Highlights
- •
Properly proportioned teeth are required for optimal occlusion and esthetics.
- •
An easy method to determine the ideal size of a missing tooth would be helpful.
- •
Formulae and a simplified chart for determining optimal tooth sizes are presented.
- •
A sample letter for communicating with restorative dentists is included.
Patients often have multifaceted and complex issues, rendering a less than optimal smile. The obligations of the orthodontist and restorative dentist are to collaboratively diagnose all functional and esthetic components of the smile, to determine achievable objectives based on the patient’s chief complaint, and to articulate a treatment plan. Various studies have mentioned several factors that seem to contribute to smile esthetics including fullness of buccal corridors, midlines, gingival architecture, tooth and gingival display during smiling and repose, and smile arc. Although each can be important in smile design, some would argue that the most essential component in creating a beautiful smile is for the patient to have ideal tooth anatomy. This article focuses on the requisite achievement of correctly sized teeth in proportion to themselves and adjacent teeth, specifically addressing the length-to-width ratio of individual teeth and their size relative to the other teeth.
To obtain an optimal occlusion, proper tooth proportions are necessary because the correct tooth mass of the maxillary and mandibular teeth permits ideal alignment in conjunction with full space closure. From an esthetic point of view, correct tooth proportions are an integral part of smile design, but many of our patients have less than ideal tooth anatomy. Anomalous and missing maxillary lateral incisors are quite common in the general population, and these teeth are most likely to vary in size between left and right, exclusive of third molars. In addition to anomalous and missing incisors, other factors that create challenges for the dentist and orthodontist when designing an esthetic and occlusally sound dentition are attrition, trauma, transposition, erosion, and caries. With all of these potential obstacles, it is critical to know ideal tooth sizes, shapes, and proportions. The orthodontist and restorative dentist need to be able to calculate the ideal size of an anomalous maxillary lateral incisor when the contralateral incisor is missing, anomalous, or out of proportion to the central incisor. Some have suggested using the golden proportion to calculate the ideal size of teeth. The golden proportion has been suggested for intra-arch tooth arrangement; however, this concept has been refuted in several studies in which patients and doctors were dissatisfied with these smile design ratios.
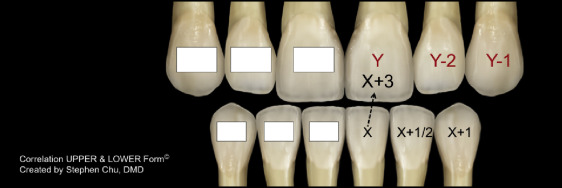
Chu determined the mean widths of anterior teeth and demonstrated that the averages only apply to 34% of the population when analyzing maxillary teeth and to 42% for mandibular teeth, whereas approximately 80% of the population have anterior tooth widths that are within 0.5 mm of the research sample mean. Furthermore, Chu showed a significant correlation between the widths of the central incisors, lateral incisors, and canines. Chu and others rounded up the widths of the teeth to the nearest 0.5 mm, stating that smaller differences in tooth width size may become clinically undetectable to the human eye. Using the correlations, dentists can quickly determine the optimal width of a missing or anomalous tooth. For the maxillary anterior teeth, given the width of the central incisor, the lateral incisor is 2 mm smaller and the canine is 1 mm smaller than the central incisor. This can be expressed with simple formulae:
Maxillary central incisor (in millimeters) = Y
Maxillary lateral incisor = Y – 2 mm
Maxillary canine = Y – 1 mm
For the mandibular teeth, given the width of the central incisor, the lateral incisor is 0.5 mm larger and the canine is 1 mm larger than the central incisor. The following equations demonstrate this relationship:
Mandibular central incisor (in millimeters) = X
Mandibular lateral incisor = X + 0.5 mm
Mandibular canine = X + 1 mm
When several anterior teeth are anomalous, missing, or not ideally sized, the width of the mandibular central incisor can be used to calculate the ideal sizes of the other teeth because it is the least variable tooth among the 12 anterior teeth. Therefore, its width can be measured to establish ideal maxillary incisor widths. This is accomplished by recognizing that the maxillary central incisor is typically 3 mm wider than the mandibular central incisor. The formula is shown below:
Y = X + 3 mm
Discussion
Figure 1 illustrates how to combine all of these formulae; this allows the clinician to determine the ideal widths of various teeth, even if the patient has several missing teeth. To make all of this easy to commit to memory, the mean size of the maxillary central incisor is 8.5 mm wide by 11 mm in length. Conveniently, the maxillary central incisor is about the same size as standard printer paper: 8.5 × 11. Although we obviously measure teeth in millimeters and paper in inches, 8.5 × 11 is certainly easy to remember. Moreover, if you commit the average size of the maxillary central incisor to memory, all of the other widths are easy to calculate using the equations provided. The average sizes of mandibular anterior teeth from central incisor to canine 5.5, 6, and 6.5 mm, respectively, yielding a total of 36 mm of mandibular anterior tooth mass. The maxillary average sizes from central incisor to canine are 8.5, 6.5, and 7.5 mm, respectively. Adding the tooth widths in this example gives a total tooth mass of 45 mm for the maxillary anterior teeth; 36 mm divided by 45 mm gives an anterior Bolton ratio of 80%, as compared with the normal anterior Bolton ratio of 77.2%. When using this outline, there will be a slight mandibular tooth excess of 1.26 mm in the anterior dentition. This may seem clinically unacceptable to some, but there is expected human error involved in the precision of measuring teeth and the accuracy of fabricating exact-sized restorations. The sum of this error may approach that of the remaining Bolton discrepancy. Additionally, the anterior Bolton ratio is most applicable in Class I skeletal malocclusions with the maxillary and mandibular incisors at a specific angulation. Given the vast array of dental and skeletal malocclusions, achieving a specific Bolton ratio is not always clinically necessary to achieve an esthetic and functionally sound occlusion.