Introduction
A multicenter parallel 3-arm randomized clinical trial was carried out in 1 university and 2 district hospitals in the United Kingdom to investigate the effect of supplemental vibrational force on orthodontically induced inflammatory root resorption (OIIRR) during the alignment phase of fixed appliance therapy.
Methods
Eighty-one subjects less than 20 years old with mandibular incisor irregularity undergoing extraction-based fixed-appliance treatment were randomly allocated to supplementary (20 minutes a day) use of an intraoral vibrational device (AcceleDent; OrthoAccel Technologies, Houston, Tex) (n = 29), an identical nonfunctional (sham) device (n = 25), or fixed appliances only (n = 27). OIIRR was measured blindly from long-cone periapical radiographs of the maxillary right central incisor taken at the start of treatment and the end of alignment when a 0.019 × 0.025-in stainless steel archwire was placed (mean follow-up, 201.6 days; 95% confidence interval [CI], 188.6-214.6 days). Data were analyzed blindly on a per-protocol basis because losses to follow-up were minimal, with descriptive statistics, 1-way analysis of variance, and univariable and multivariable regression modeling.
Results
Nine patients were excluded from the analysis; they were evenly distributed across the groups. Mean overall OIIRR measured among the 72 patients was 1.08 mm (95% CI, 0.89-1.27 mm). Multivariable regression indicated no significant difference in OIIRR for the AcceleDent (difference, 0.22 mm; 95% CI, −0.14-0.72; P = 0.184) and AcceleDent sham groups (difference, 0.29 mm; 95% CI, −0.15-0.99; P = 0.147) compared with the fixed-appliance-only group, after accounting for patient sex, age, malocclusion, extraction pattern, alignment time, maximum pain experienced, history of dentoalveolar trauma, and initial root length of the maxillary right central incisor. No other side-effects were recorded apart from pain and OIIRR.
Conclusions
The use of supplemental vibrational force during the alignment phase of fixed appliance orthodontic treatment does not affect OIIRR associated with the maxillary central incisor.
Registration
ClinicalTrials.gov ( NCT02314975 ).
Protocol
The protocol was not published before trial commencement.
Funding
Functional and sham AcceleDent units were donated by the manufacturer; there was no contribution to the conduct or the writing of this study.
Graphical abstract
Highlights
- •
It has been claimed that vibrational force can accelerate orthodontic tooth movement.
- •
Root resorption is a common consequence of treatment with fixed appliances.
- •
We studied the effect of vibration on root resorption with fixed appliances.
- •
We randomized 81 patients with fixed appliance to vibration, placebo, or neither.
- •
Vibrational force does not influence root resorption during fixed appliance alignment.
- •
The proportions of patients with severe root resorption were similar in the 3 groups.
Orthodontically induced inflammatory root resorption (OIIRR) is a common pathologic side effect of orthodontic treatment with fixed appliances and is the consequence of a multifactorial sterile inflammation in the periodontal ligament. The prevalence of OIIRR among orthodontic patients has been reported as 73%, 90%, and 100% in studies using plain film radiographs, cone-beam computed tomography (CBCT), and histology, respectively. OIIRR most commonly affects the maxillary incisors, mandibular incisors, and permanent first molars and is usually mild, with only about 16% of orthodontic patients having clinically relevant shortening of at least 1 tooth root.
The etiology of OIIRR is believed to be multifactorial, with many factors influencing outcome, including root morphology, history of dentoalveolar trauma, patient age, and any underlying systemic inflammatory condition, such as asthma or allergy. Factors related to orthodontic treatment include the level and direction of force, the type of force, and contact of tooth roots with cortical bone. However, the specific role relating to many of these factors is poorly understood, and there is only good evidence that heavier orthodontic forces cause greater OIIRR than do light forces, and that increased treatment time positively correlates to increased OIIRR.
The increased risk of OIIRR in association with prolonged orthodontic tooth movement makes shorter treatment a worthwhile goal. The use of supplemental vibrational force has recently been advocated as a method of accelerating orthodontic tooth movement and reducing overall treatment time. Vibrational force has long been recognized as anabolic for bone, having been used to potentially increase bone mass in astronauts exposed to prolonged periods of microgravity and in terrestrials susceptible to bone loss, such as postmenopausal women and those confined to a wheelchair or bed. In animal models, vibrational force has been shown to promote bony remodeling at sutures and speed up orthodontic tooth movement. Based on these data, several devices have been developed that are now commercially available and designed to deliver vibrational force directly to the dentition. One of these, AcceleDent (OrthoAccel Technologies, Houston, Tex), is a hands-free removable portable appliance consisting of an activator unit and a mouthpiece; it provides a vibrational frequency of 30 Hz and a force of 0.2 N. The patient bites gently onto a vibrating thermoplastic wafer, which is in contact with the occlusal surface of both the maxillary and mandibular dentitions. The patient uses the appliance for a recommended 20 minutes per day, and it is claimed that this will result in an acceleration of tooth movement and an overall reduction in orthodontic treatment time.
There are currently data from retrospective studies and 2 randomized clinical trials showing evidence of increased rates of tooth movement and reduced pain when using fixed appliances combined with supplemental vibrational force. However, retrospective studies are known to be associated with bias and exaggeration of treatment effects, and both randomized trials were at risk of bias. Advertisement claims and the promising results of the early pilot studies have not been confirmed by subsequent well-designed randomized clinical trials; these have shown no improvement in either tooth alignment rate or pain experience associated with supplemental vibrational force. Importantly, no studies have so far reported on whether the use of supplemental vibrational force has any impact on the levels of OIIRR experienced by patients undergoing orthodontic treatment with fixed appliances. The only trial to date on OIIRR is a small pilot split-mouth randomized trial with 15 patients; the authors found that AcceleDent had no significant effect on the total volume of root resorption associated with the first premolars in a 4-week period. However, the follow-up associated with this small unpublished study was too short to provide any significant data. See Supplemental Materials for a short video presentation about this study.
Specific objectives and hypotheses
The aim of this randomized clinical trial report was to investigate OIIRR experienced during tooth alignment with fixed orthodontic appliances supplemented with vibrational force provided by the AcceleDent appliance. The null hypothesis was that supplemental vibrational force does not affect the levels of OIIRR during the alignment phase of orthodontic treatment with fixed appliances.
Material and methods
Trial design and changes after trial commencement
This was a 3-arm parallel randomized controlled trial comparing the effects of supplemental vibrational force on OIIRR in adolescent patients undergoing orthodontic treatment with premolar extractions and fixed appliances in 3 centers in the United Kingdom. Ethical approval was obtained from the United Kingdom National Research Ethics Service (South East London REC 3, 11/LO/0056), and written informed consent was received from all parents, guardians, and children. All methods were performed in accordance with the approved guidelines and regulations. The trial was registered at the European Clinical Trials Database (EudraCT, 2014-004211-37) on September 29, 2014, and ClinicalTrials.gov ( NCT02314975 ) on November 25, 2014. No changes to the methodology occurred after trial commencement. The data are presented according to the CONSORT statement.
Participants, eligibility criteria, and settings
Participants were recruited from patients referred to the orthodontic departments at King’s College London Dental Institute (Guy’s Hospital); Royal Alexander Children’s Hospital, Brighton; and William Harvey Hospital, Ashford, between July 2011 and May 2014. The former is based in a dental school, and the others are based in district general hospitals. All provide comprehensive orthodontic services and treatment. The inclusion criteria related to the trial primary outcome were (1) under 20 years of age at treatment start; (2) no medical contraindications, including regular medication; (3) permanent dentition; (4) mandibular arch incisor irregularity; and (5) extraction of mandibular premolars as part of the orthodontic treatment plan. Patients who fulfilled these criteria were invited to join and consented appropriately.
Interventions
Participants were randomly allocated to 1 of 3 treatment groups: (1) preadjusted edgewise fixed appliance treatment with adjunctive daily use of a functional AcceleDent (OrthoAccel Technologies) vibrational device (Accel group), (2) preadjusted edgewise fixed appliance treatment with adjunctive use of a nonfunctional (sham) AcceleDent device (Accel-sham group), and (3) preadjusted edgewise fixed appliance treatment alone (fixed-only group). Subjects allocated to the functional and sham devices were given direct verbal and written instructions on operation and usage, and instructed to use the device for 20 minutes per day as per the manufacturer. They were also shown the electronic timer and therefore made aware that their compliance was being monitored. The sham device was identical to the active device in all respects, except that it did not vibrate when switched on. The fixed appliance used was standardized between groups (MBT prescription 0.022-in precoated Victory series; 3M Unitek, Monrovia, Calif) as was the archwire sequence used for the alignment phase of treatment: 0.014-in, 0.018-in, 0.018 × 0.025-in nickel-titanium, and 0.019 × 0.025-in stainless steel archwires. The dental arches were bonded from the first molars, and the archwires were ligated fully with conventional elastomeric ligation. After the initial placement of the appliances, patients were seen approximately every 8 weeks. Progression into the next archwire occurred only when the previous archwire had become passive and the new archwire could be fully ligated into the bracket slot. The archwires were cut distal to the first molars and were not cinched. No bite planes, auxiliary arches, intermaxillary elastics, headgears, or temporary anchorage devices were used during the period of investigation. All subjects were treated by senior orthodontists (A.T.D., N.J., C.S., and J.G.) or experienced orthodontic residents (N.R.W. and M.A.) under their direct supervision.
Outcomes
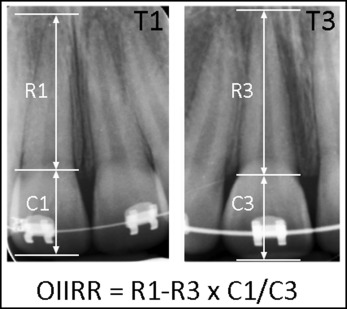
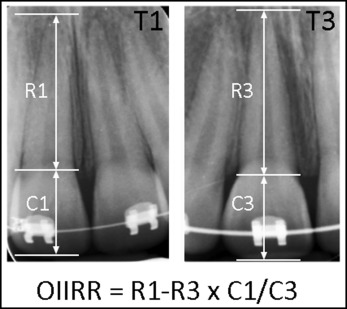
The main outcome for this report was the amount of OIIRR that occurred during the alignment phase of treatment using fixed orthodontic appliances, as measured from the maxillary right central incisor. This was planned as a secondary outcome of a randomized trial with the primary outcome the tooth alignment rate. Specifically, OIIRR was measured from long-cone periapical radiographs (LCPAs) taken at the start of treatment (T1) and at the end of alignment on insertion of a 0.019 × 0.025-in stainless steel archwire (T3). Measurements were made directly from the scanned radiographs with Adobe Photoshop CS3 (version 10; Adobe Systems, San Jose, Calif) using the ruler tool to the nearest 0.1 mm by 1 operator (A.T.D.) who was blinded to the patient’s group. The difference in root length from the LCPAs taken at T1 and T3 was determined using a correction factor to account for differences in enlargement between the 2 films based on the measured crown length ( Fig 1 ). There were no changes to outcomes after trial commencement.
An additional outcome was the number of patients with severe OIIRR, which was defined in this study as OIIRR greater than 2 mm measured from the LCPAs.
Data on maximum pain on a 100-mm visual analog scale and analgesic use during the initial alignment phase were available from a previous trial report, and the prevalence of dentoalveolar trauma on the maxillary incisors was assessed through patient history and clinical or radiographic examinations. Both of these factors were used as covariates in the analyses.
Sample size calculation
The sample size calculation for this trial was based on the primary outcome of the initial rate of orthodontic tooth alignment, which gave a required sample of 23 patients per group and has been described previously. A previous investigation of OIIRR differences between 2 bracket systems adopted a difference of 0.4 mm as clinically significant to calculate sample size. A post hoc power calculation after code breaking for the secondary outcome of OIIRR, using the above mentioned difference, gave a root mean squared error incorporating the variance of the OIIRR from this trial, and a 5% level of significance indicated that it would have a power of 25% to 30%.
Randomization
The randomization sequence was generated by an investigator (M.T.C.) using GraphPad online software ( http://www.graphpad.com/quickcalcs/index.cfm ) with unrestricted equal participant allocation (1:1:1) and undertaken centrally at King’s College London, independently from the clinical operators, after recruitment (allocation concealment).
Blinding
Although the treating clinicians and subjects could not be blinded to the use of AcceleDent, the subjects were not told whether they were allocated to a functional or a sham appliance; these were identical in appearance, although the sham appliance did not vibrate. The extracted data including the LCPAs were coded, so that both the outcome assessor (A.T.D.) and the statistician (S.N.P.) were blinded to subject allocation. The coding of the data was broken after the end of the analysis, and no breach of blinding was identified.
Statistical analysis
Conventional descriptive statistics, including means and standard deviations were used to present the demographic data for each group, whereas differences between the groups were assessed using analysis of variance (ANOVA) for continuous data and the chi-square test for binary data, after checking for homoscedacity and normality of residuals. Regression modeling was carried out to assess the influence of the intervention on the 2 secondary outcomes of this trial, both individually using univariable modeling and collectively using multivariable modeling. Generalized linear models and their extensions to the binomial family were used, estimating relative risks rather than odds ratios for the latter, because of their advantages. Multivariable analyses included all possible confounders, including initial root length, malocclusion type, extraction pattern, alignment duration, maximum pain reported from the patient during alignment, use of painkillers during alignment, and history of dentoalveolar trauma during the alignment phase.
Reproducibility of the measurements was determined by repeated measurements of 20 sets of radiographs made 2 weeks apart from the same outcome assessor (A.T.D.) by calculating the intraclass correlation coeffient (ICC), the average difference of the 2 readings, and the 95% limits of agreement according to the Bland-Altman method. A 2-tailed P value of 0.05 was considered statistically significant with a 95% confidence interval (CI) for all tests. All analyses were carried out before code breaking using Stata software (version 12.0; StataCorp, College Station, Tex) by1 person (S.N.P.) blinded to the allocation, except for the post hoc power calculation, which was conducted after code breaking.
Material and methods
Trial design and changes after trial commencement
This was a 3-arm parallel randomized controlled trial comparing the effects of supplemental vibrational force on OIIRR in adolescent patients undergoing orthodontic treatment with premolar extractions and fixed appliances in 3 centers in the United Kingdom. Ethical approval was obtained from the United Kingdom National Research Ethics Service (South East London REC 3, 11/LO/0056), and written informed consent was received from all parents, guardians, and children. All methods were performed in accordance with the approved guidelines and regulations. The trial was registered at the European Clinical Trials Database (EudraCT, 2014-004211-37) on September 29, 2014, and ClinicalTrials.gov ( NCT02314975 ) on November 25, 2014. No changes to the methodology occurred after trial commencement. The data are presented according to the CONSORT statement.
Participants, eligibility criteria, and settings
Participants were recruited from patients referred to the orthodontic departments at King’s College London Dental Institute (Guy’s Hospital); Royal Alexander Children’s Hospital, Brighton; and William Harvey Hospital, Ashford, between July 2011 and May 2014. The former is based in a dental school, and the others are based in district general hospitals. All provide comprehensive orthodontic services and treatment. The inclusion criteria related to the trial primary outcome were (1) under 20 years of age at treatment start; (2) no medical contraindications, including regular medication; (3) permanent dentition; (4) mandibular arch incisor irregularity; and (5) extraction of mandibular premolars as part of the orthodontic treatment plan. Patients who fulfilled these criteria were invited to join and consented appropriately.
Interventions
Participants were randomly allocated to 1 of 3 treatment groups: (1) preadjusted edgewise fixed appliance treatment with adjunctive daily use of a functional AcceleDent (OrthoAccel Technologies) vibrational device (Accel group), (2) preadjusted edgewise fixed appliance treatment with adjunctive use of a nonfunctional (sham) AcceleDent device (Accel-sham group), and (3) preadjusted edgewise fixed appliance treatment alone (fixed-only group). Subjects allocated to the functional and sham devices were given direct verbal and written instructions on operation and usage, and instructed to use the device for 20 minutes per day as per the manufacturer. They were also shown the electronic timer and therefore made aware that their compliance was being monitored. The sham device was identical to the active device in all respects, except that it did not vibrate when switched on. The fixed appliance used was standardized between groups (MBT prescription 0.022-in precoated Victory series; 3M Unitek, Monrovia, Calif) as was the archwire sequence used for the alignment phase of treatment: 0.014-in, 0.018-in, 0.018 × 0.025-in nickel-titanium, and 0.019 × 0.025-in stainless steel archwires. The dental arches were bonded from the first molars, and the archwires were ligated fully with conventional elastomeric ligation. After the initial placement of the appliances, patients were seen approximately every 8 weeks. Progression into the next archwire occurred only when the previous archwire had become passive and the new archwire could be fully ligated into the bracket slot. The archwires were cut distal to the first molars and were not cinched. No bite planes, auxiliary arches, intermaxillary elastics, headgears, or temporary anchorage devices were used during the period of investigation. All subjects were treated by senior orthodontists (A.T.D., N.J., C.S., and J.G.) or experienced orthodontic residents (N.R.W. and M.A.) under their direct supervision.
Outcomes
The main outcome for this report was the amount of OIIRR that occurred during the alignment phase of treatment using fixed orthodontic appliances, as measured from the maxillary right central incisor. This was planned as a secondary outcome of a randomized trial with the primary outcome the tooth alignment rate. Specifically, OIIRR was measured from long-cone periapical radiographs (LCPAs) taken at the start of treatment (T1) and at the end of alignment on insertion of a 0.019 × 0.025-in stainless steel archwire (T3). Measurements were made directly from the scanned radiographs with Adobe Photoshop CS3 (version 10; Adobe Systems, San Jose, Calif) using the ruler tool to the nearest 0.1 mm by 1 operator (A.T.D.) who was blinded to the patient’s group. The difference in root length from the LCPAs taken at T1 and T3 was determined using a correction factor to account for differences in enlargement between the 2 films based on the measured crown length ( Fig 1 ). There were no changes to outcomes after trial commencement.
An additional outcome was the number of patients with severe OIIRR, which was defined in this study as OIIRR greater than 2 mm measured from the LCPAs.
Data on maximum pain on a 100-mm visual analog scale and analgesic use during the initial alignment phase were available from a previous trial report, and the prevalence of dentoalveolar trauma on the maxillary incisors was assessed through patient history and clinical or radiographic examinations. Both of these factors were used as covariates in the analyses.
Sample size calculation
The sample size calculation for this trial was based on the primary outcome of the initial rate of orthodontic tooth alignment, which gave a required sample of 23 patients per group and has been described previously. A previous investigation of OIIRR differences between 2 bracket systems adopted a difference of 0.4 mm as clinically significant to calculate sample size. A post hoc power calculation after code breaking for the secondary outcome of OIIRR, using the above mentioned difference, gave a root mean squared error incorporating the variance of the OIIRR from this trial, and a 5% level of significance indicated that it would have a power of 25% to 30%.
Randomization
The randomization sequence was generated by an investigator (M.T.C.) using GraphPad online software ( http://www.graphpad.com/quickcalcs/index.cfm ) with unrestricted equal participant allocation (1:1:1) and undertaken centrally at King’s College London, independently from the clinical operators, after recruitment (allocation concealment).
Blinding
Although the treating clinicians and subjects could not be blinded to the use of AcceleDent, the subjects were not told whether they were allocated to a functional or a sham appliance; these were identical in appearance, although the sham appliance did not vibrate. The extracted data including the LCPAs were coded, so that both the outcome assessor (A.T.D.) and the statistician (S.N.P.) were blinded to subject allocation. The coding of the data was broken after the end of the analysis, and no breach of blinding was identified.
Statistical analysis
Conventional descriptive statistics, including means and standard deviations were used to present the demographic data for each group, whereas differences between the groups were assessed using analysis of variance (ANOVA) for continuous data and the chi-square test for binary data, after checking for homoscedacity and normality of residuals. Regression modeling was carried out to assess the influence of the intervention on the 2 secondary outcomes of this trial, both individually using univariable modeling and collectively using multivariable modeling. Generalized linear models and their extensions to the binomial family were used, estimating relative risks rather than odds ratios for the latter, because of their advantages. Multivariable analyses included all possible confounders, including initial root length, malocclusion type, extraction pattern, alignment duration, maximum pain reported from the patient during alignment, use of painkillers during alignment, and history of dentoalveolar trauma during the alignment phase.
Reproducibility of the measurements was determined by repeated measurements of 20 sets of radiographs made 2 weeks apart from the same outcome assessor (A.T.D.) by calculating the intraclass correlation coeffient (ICC), the average difference of the 2 readings, and the 95% limits of agreement according to the Bland-Altman method. A 2-tailed P value of 0.05 was considered statistically significant with a 95% confidence interval (CI) for all tests. All analyses were carried out before code breaking using Stata software (version 12.0; StataCorp, College Station, Tex) by1 person (S.N.P.) blinded to the allocation, except for the post hoc power calculation, which was conducted after code breaking.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


