Introduction
Our aims in this study were to assess the prevalence of severe root resorption and identify possible associations in orthodontic patients treated with the edgewise method.
Methods
The sample included 1049 patients who had periapical radiographs taken for all incisors before and after treatment. The radiographs were examined by 2 orthodontists using an x-ray viewer with standard light intensity. These variables were collected: root shape, overbite, initial resorption, and hypodontia. The patients were classified according to sex, Angle classification, ethnicity, age, duration of treatment, type of dentition (mixed or permanent), and treatment with or without extraction of 4 premolars. Resorption was considered severe when it affected more than a third of the length of the root. Statistical analysis included the chi-square test and both simple and multiple logistic regression ( P ≤0.05).
Results
Severe root resorption was observed in 14.5% of the sample. Patients treated with exodontia of the first premolars (odds ratio [95% CI] = 6.38 [4.2-9.7]), those who had triangle-shaped roots at the beginning of treatment (odds ratio [95% CI] = 4.67 [3.1-6.9]), and those with initial root resorption (odds ratio [95% CI] = 4.52 [2.7-7.6]) had a greater chance of developing severe root resorption during orthodontic treatment.
Conclusions
A high prevalence of severe root resorption was observed in Brazilian patients treated with the edgewise method. The main factors directly involved in severe resorption were extraction of first premolars, triangle-shaped roots, and root resorption before treatment.
Evidence in the literature does not yet allow orthodontists to precisely predict the interaction between orthodontic treatment and root resorption. Individual predisposition, familial association, racial factors, allergies and asthma, magnitude and direction of maxillary incisor displacement, and teeth with blunt or pipette-shaped roots are considered risk factors for root resorption during orthodontic treatment. However, no definitive conclusion has been drawn as to whether sex, age, tooth extractions, and duration of active treatment are risk factors for root resorption. Conflicting data are reported on the relationship between root resorption and hypodontia or partial anodontia and ectopic teeth.
From a critical assessment of the literature, it is difficult to determine precisely the contribution of each related variable. Part of this difficulty can be explained by various methodologic criteria used in studies, different sample sizes, and the heterogeneity of study populations. Thus, results have been conflicting, thereby compromising their credibility and clinical application. Furthermore, although severe and very severe root resorption can cause drastic consequences to both the treatment and the patient’s health, no studies specifically address the risk factors for these conditions.
In cases of extensive root resorption induced by orthodontic movement, there might be flaws in the predictability, prevention, and early diagnosis of this condition. It is therefore important to determine the magnitude and prevalence of root resorption in various populations as well as related risk factors.
The aims of this retrospective study were to determine the prevalence of severe root resorption (more than a third of the length of the root) in Brazilian patients treated with the edgewise method and the relationship between severe resorption and other treatment-related variables.
Material and methods
A total of 1154 patient files were examined from which 105 were excluded, leaving a sample of 1049 patients (12,588 periapical radiographs; 12 per patient, 6 pretreatment and 6 posttreatment) with a mean age of 12.1 years (SD, 1.7) at the beginning of treatment. All patients were treated with pure edgewise mechanics at the Postgraduate Orthodontics Clinic at the Dental School of the Federal University of Rio de Janeiro, Brazil. The selection criteria excluded patients with a prior history of dental trauma, endodontic treatment, nail-biting, other habits, and radiographic signs of pathologies. Patients whose treatment had not been completed were also excluded, and poor-quality radiographs were eliminated from the study. No patient was being retreated. Demographic information (age at beginning of treatment and sex), pretreatment diagnosis, and treatment information were obtained for all patients from the charts and records.
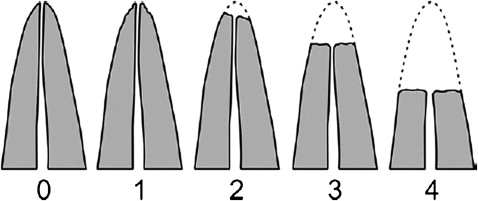
To assess resorption, pretreatment and posttreatment periapical radiographs of the maxillary and mandibular incisors were assessed by 2 examiners (L.S.M. and A.C.R.) in an x-ray viewer with standard light intensity. The incisors were selected to represent root resorption because they are considered the most prone to this condition during treatment. The estimated projection error was evaluated in 105 randomly selected patients. Using the method proposed by Baumrind et al., the mean error was 0.03 mm (SD, 0.09; range, –0.11-0.18 mm; intraclass correlation coefficient, 0.99). Radiographic distortion was too insignificant to cause diagnostic errors regarding severe root resorption. Signs of apical root resorption were registered with index scores from 0 to 4: 0, no resorption; 1, irregular root contour; 2, apical root resorption less than 2 mm; 3, apical root resorption from 2 mm to a third of the original root length; and 4, root resorption exceeding a third of the original root length ( Fig ). A calibration exercise was carried out on a random selection of 10% of all radiographs. Intraexaminer and interexaminer scores for the measures of agreement calculated on a tooth-by-tooth basis were high (minimum weighted kappa values were 0.93 and 0.88, respectively).
The outcome variable, severe root resorption, was dichotomized as yes for patients with at least 1 tooth in stage 4 (root resorption exceeding a third of the original root length) and no for patients without resorption or those with stages 1 to 3 resorption. The following variables were assessed: root shape, overbite, initial resorption, and hypodontia. The patients were classified with regard to sex, Angle classification, ethnicity, age, duration of treatment, type of dentition (mixed or permanent), and treatment with or without extraction of 4 first premolars. Panoramic radiographs were analyzed for hypodontia and other dental development anomalies.
Statistical analysis
The results were organized and entered into a data bank by using the Statistical Package for Social Science software (version 14.0, SPSS, Chicago, Ill). For the statistical analysis, we initially described the absolute and relative frequencies of the variables studied. Associations were then tested by using univariate analysis between the independent variables and the outcome (chi-square test). An association between variables (significance, >0.05) was considered as the null hypothesis. To determine the chances of root resorption, variables with a P value ≤0.010 in the univariate analysis were included 1 by 1 in the multiple logistic regression model. The final model was adjusted for the effect of all variables. The odds ratio and 95% confidence intervals were estimated for each variable in the logistic model.
Results
The prevalence of severe root resorption was 14.5% (n = 152). Table I shows the distribution of the variables for presence or absence of severe resorption. Statistically significant differences were observed between the outcome (severe root resorption) and the following independent variables: treatment type (with or without extraction of first premolars), root shape (pointed or normal), and resorption before orthodontic treatment.
| Severe root resorption | ||||
|---|---|---|---|---|
| Variable | Present n (%) | Absent n (%) | Total | P |
| Sex | ||||
| Female | 81 (13.9) | 500 (86.1) | 581 (100) | 0.574 |
| Male | 71 (15.2) | 397 (84.8) | 468 (100) | |
| Age | ||||
| ≥12 years | 66 (14.3) | 397 (85.7) | 463 (100) | 0.848 |
| <12 years | 86 (14.7) | 500 (85.3) | 586 (100) | |
| Treatment time | ||||
| >3 years | 27 (12.9) | 182 (87.1) | 209 (100) | 0.471 |
| ≤3 years | 125 (14.9) | 715 (85.1) | 840 (100) | |
| Dentition | ||||
| Mixed | 90 (14.8) | 520 (85.2) | 610 (100) | 0.775 |
| Permanent | 62 (14.1) | 377 (85.9) | 439 (100) | |
| Overbite | ||||
| ≥4 mm | 20 (14.0) | 123 (86.0) | 143 (100) | 0.854 |
| <4 mm | 132 (14.6) | 774 (85.4) | 906 (100) | |
| Class I | ||||
| Present | 49 (13.0) | 329 (87.0) | 378 (100) | 0.292 |
| Other malocclusions | 103 (15.4) | 568 (84.6) | 671 (100) | |
| Class II Division 1 | ||||
| Present | 84 (16.5) | 426 (83.5) | 510 (100) | 0.076 |
| Other malocclusions | 68 (12.6) | 471 (87.4) | 539 (100) | |
| Class II Division 2 | ||||
| Present | 16 (13.1) | 106 (86.9) | 122 (100) | 0.646 |
| Other malocclusions | 136 (14.7) | 791 (85.3) | 927 (100) | |
| Class III | ||||
| Present | 3 (7.9) | 106 (86.9) | 38 (100) | 0.239 |
| Other malocclusions | 149 (14.7) | 791 (85.3) | 1011 (100) | |
| Treatment with exodontia of 4 first premolars | ||||
| Yes | 115 (28.9) | 283 (71.1) | 398 (100) | 0.000 |
| No | 37 (5.7) | 614 (94.3) | 651 (100) | |
| Root shape | ||||
| Triangular | 99 (31.5) | 215 (68.5) | 314 (100) | 0.000 |
| Rhomboidal | 53 (7.2) | 682 (92.8) | 735 (100) | |
| Initial resorption | ||||
| Present | 45 (46.9) | 51 (53.1) | 67 (100) | 0.000 |
| Absent | 107 (11.2) | 846 (88.8) | 982 (100) | |
| Hypodontia | ||||
| Present | 17 (17.7) | 79 (82.3) | 96 (100) | 0.347 |
| Absent | 135 (14.2) | 818 (85.8) | 953 (100) | |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


