Introduction
The aim of this study was to analyze 3-dimensional data of root morphology and development in labial inversely impacted maxillary central incisors.
Methods
Cone-beam computed tomography images from 41 patients with impacted incisors were divided into early and late dental age groups according to their dental age. Sagittal slices in which the labiolingual width of the tooth was the widest in the axial view were evaluated. The inverse angle, the dilaceration angle, and the length of both impacted and homonym teeth were evaluated with SimPlant Pro software (version 13.0; Materialise Dental NV, Leuven, Belgium).
Results
The Student t test indicated that the lengths of the impacted teeth were significantly shorter than those of the homonym teeth ( P <0.05), and the root lengths of the early dental age group were significantly shorter than those of the late dental age group. The results from chi-square tests indicated that the incidence of dilacerations was significantly higher in the late dental age group when compared with the early dental age group. Multiple regression analyses indicated that the independent variables for root length of the impacted teeth were dental age (β = 0.958; P <0.001) and length of the nondilacerated part of the root (β = 0.435; P <0.001).
Conclusions
Dilaceration was more common in the late dental age group. The roots of labial inversely impacted maxillary central incisors continue developing, but their potential is limited.
Highlights
- •
We examined CBCT images from 41 patients with labial inversely impacted incisors.
- •
Patients were divided into early and late dental age groups according to their dental age.
- •
Inverse angle, dilaceration angle, and root length were evaluated by SimPlant.
- •
The incidence of dilacerations was significantly higher in the late group.
- •
The roots of impacted incisors continue developing, but their potential is limited.
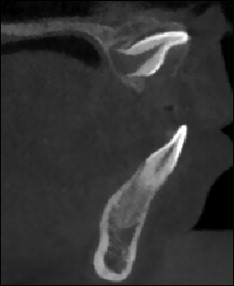
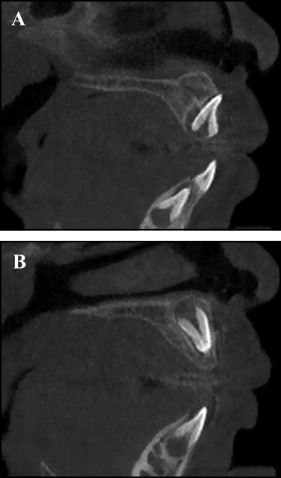
A labial inversely impacted maxillary central incisor is regarded as the most complicated type of impacted tooth, with its crown directing upward and the palatal aspect of the crown facing labially. Because of the elevated position of the crown, the success rate of correction for a labial inversely impacted maxillary central incisor is relatively low. Figure 1 is based on images of sagittal slices obtained by cone-beam computed tomography (CBCT). Dilaceration, defined as an angulation in the linear relationship of the crown to the root, is often observed in patients with labial inversely impacted incisors. Impacted teeth lead to serious problems such as irregular dentition, diastema, incisor transposition, and root resorption of adjacent teeth.
In addition to a routine clinical examination, a radiographic examination is essential in diagnosing root morphology, development, and dilaceration. Conventionally, radiographic diagnosis was based on 2-dimensional (2D) radiographic images. However, 2D radiographic images can be hindered by rotation, distortion, and errors in head positioning, which cause inaccurate representations of anatomic landmarks and poor visualization of some anatomic structures. CBCT has been recently introduced in radiographic diagnosis of impacted teeth, since it provides multiple planes for accurately identifying 3-dimensional (3D) landmarks of dental structures with submillimeter resolution. CBCT also provides various sections of the structure of interest, allowing clinicians to assess the exact positions of the apex and the crown, and the degrees of root formation and dilaceration. A previous study demonstrated that 3D surface models derived from CBCT are sufficiently precise and accurate when compared with physical measurements made directly on skulls. The advantages of CBCT over conventional computed tomography or dental images include low radiation dose, low cost, excellent tissue contrast, elimination of blurring and overlapping of adjacent teeth, and high spatial resolution. Therefore, the application of CBCT in the diagnosis and treatment of impacted teeth has become increasingly indispensable.
Studies of labial inversely impacted maxillary central incisors were found mainly in case reports, most of which were limited in scope because of sole reliance on 2D radiographic images for analyzing root morphology and length of impacted teeth. To determine the appropriate age to begin treatment and methods for treating inversely impacted incisors, 3D data are needed to simultaneously and systematically analyze both the development and the morphology of impacted teeth. Thus, the aim of this retrospective study was to comprehensively analyze root morphology and development in 41 patients with labial inversely impacted maxillary central incisors in the mixed dentition. A CBCT system was used in pretreatment analysis and diagnostic workup.
Material and methods
This was a retrospective observational study; 41 patients (19 boys, 22 girls; mean age, 8.69 ± 1.36 years) with labial inversely impacted maxillary central incisors, who came for treatment at the orthodontic department, Hospital of Stomatology, Wenzhou Medical University in China, were selected for this study. The method of Nolla was used to determine the dental age of all subjects. Briefly, a tooth with a third of its root formation (stage 7) or two thirds of its root formation (stage 8) was assigned to the early dental age group, and a tooth with an almost complete root but an open apex (stage 9) or completion of the root’s apical end (stage 10) was assigned to the late dental age group, as previously described.
The inclusion criteria for this study were (1) patients with full clinical documentation, including contact information and medical history (eg, dental trauma and dental treatment history); (2) all CBCT images with good definition to ensure accuracy of measurements; (3) patients with a preliminary diagnosis of maxillary inversely impacted incisors in the mixed dentition; (4) inverse tooth defined as a tooth with an angulation of the long axis of the crown to the palatal plane greater than 0° (as indicated in Figure 2 , the angle PNS-ANS-UI-WM should be greater than 0°) and homonym teeth with normal root formation and orientation; (5) permission obtained from the ethical committee for the clinical trial from the Hospital of Stomatology of Wenzhou Medical University; and (6) informed consent signed for all patients. The exclusion criteria were (1) serious oral and maxillofacial diseases other than labial inversely impacted maxillary central incisors; (2) CBCT images not taken at the Hospital of Stomatology of Wenzhou University; and (3) any systemic disease.
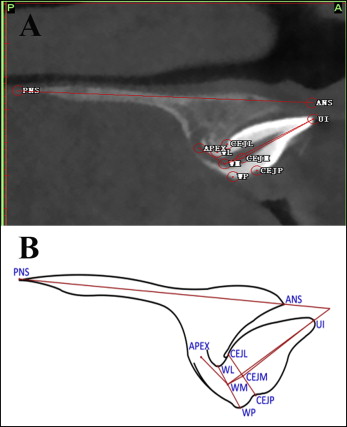
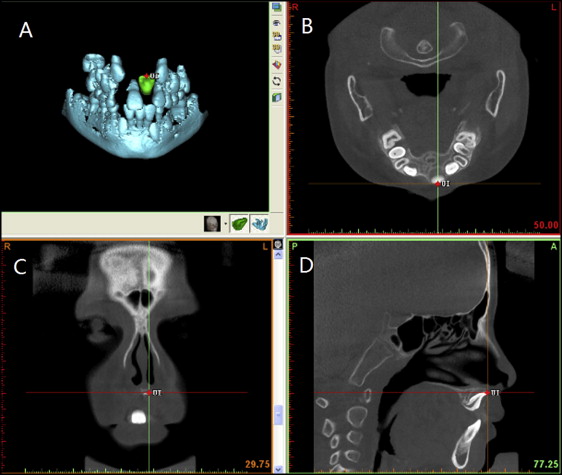
Three-dimensional CBCT scans were made during the preliminary diagnosis with a NewTom device (QR s.r.l., Verona, Italy). The typical imaging protocols were as follows: 110 kV, 1-20 mA (pulse mode), 26-second scanning time with an axial thickness of 0.25 mm; the field of view was 15 × 15 cm, and the voxel size was 0.30 × 0.25 mm. The data generated from the NNT Workstation (QR s.r.l.) software in DICOM format were imported into the SimPlant Pro program (version 13.0; Materialise Dental NV, Leuven, Belgium) for 3D reconstruction. The landmarks were established as previously described, and a total of 10 landmarks were selected and are described in Figure 2 and Table I . Sagittal slices were evaluated where the maxillary central incisor was widest labiolingually in the axial view, as described in a previous study. If the observer had difficulty visualizing any landmark in a specific plane, the computer-aided oral and maxillofacial surgery module in SimPlant was used to zoom into any plane to facilitate location of the landmark from the sagittal, coronal, and axial slices simultaneously ( Fig 3 ).
| Reference point | Definition |
|---|---|
| UI | Incisal edge of the maxillary central incisor |
| CEJL | Cementoenamel junction (CEJ) at the labial side |
| CEJP | CEJ at the palatal side |
| CEJM | Middle point of the line connecting CEJL and CEJP |
| WL | Dilaceration point at the labial side |
| WP | Dilaceration point at the palatal side |
| WM ∗ | Middle point of the line connecting WL and WP |
| APEX | Root apex of the maxillary central insicor |
| ANS | Median, sharp bony process of the maxilla |
| PNS | Sharp bony process of the hard palate |
∗ If the dilaceration occurs at the cementoenamel junction, CEJM and WM are the same point.
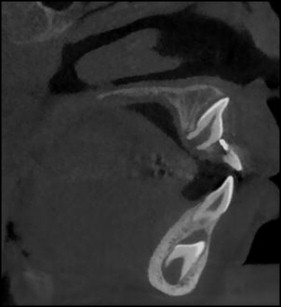
Measurements were made for variations including dental age, root and crown length of the impacted and homonym teeth, inverse angles, and dilaceration angles ( Table II ). If the dilaceration occurred along the root, the root length was divided into 2 parts: the nondilacerated root length and the dilacerated root length ( Fig 2 ). In subjects with no dilaceration, the nondilacerated root length was the same as root length ( Fig 4 ).
| Measurement variable | Definitions |
|---|---|
| Dental age | Amount of root formation |
| Inverse angle | Anterior upper angle between the long the axis of the crown and palatal plane, ∠PNS-ANS-UI-CEJM |
| Dilaceration angle | Angle between the 2 dilacerated parts of the root, ∠UI-WM-APEX |
| Crown length | Distance from UI to CEJM |
| Root length ∗ | Distance from CEJM to APEX |
| Length of nondilaceration part of root | Distance from CEJM to WM |
∗ If the dilaceration occurs at the root, the root length includes 2 parts ( Fig 2 ).
Statistical analysis
All subjects were measured twice within 10 days by the same examiner (H.S.), and the mean value was used for statistical analysis. The intraexaminer error between the 2 measurements was determined by the intraclass correlation coefficient (ICC) based on a 2-way mixed analysis of variance (ANOVA). Descriptive statistics were expressed as means and standard deviations. The paired t test was used to compare the values between the root lengths of the impacted and homonym teeth, and the 2-sample t test was used to compare the measurement variables between the early and late dental age groups. Multiple linear regression analysis was carried out to evaluate the associations between root length and the covariates (dental age, inverse and dilaceration angles, length of the nondilacerated part of the roots). Variables with a P value less than 0.05 were considered significant in the multiple regression analysis using the step-back method. The chi-square test was used for comparison of the percentages of dilacerations between the 2 groups. All statistical analyses were performed with SPSS statistical software (version 17.0; SPSS, Chicago, Ill).
Results
For 1 patient, the dental age was at stage 6, with no root formation of impacted and homonym teeth ( Fig 5 ); therefore, this patient was excluded from all statistical analyses.
The ICC values (0.78-0.98) indicated good intraexaminer reliability. As shown in Table III , the 2-sample t test indicated significant differences between the early and late dental age groups in dilaceration angles, root lengths of the impacted teeth, and root lengths of the homonym teeth ( P <0.05). In addition, the root lengths of the impacted teeth were significantly shorter than those of the homonym teeth in both the early and late dental age groups ( P <0.05) ( Table IV ).
| Measurement variable | ICC | Early dental age group (n = 18) | Late dental age group (n = 22) | Total (n = 40) | P |
|---|---|---|---|---|---|
| Dental age | NA | 7.50 ± 0.51 | 9.55 ± 0.51 | 8.63 ± 1.15 | <0.001 ∗ |
| Inverse angle (°) | 0.98 | 38.59 ± 17.64 | 45.09 ± 20.98 | 42.17 ± 19.58 | 0.293 |
| Dilaceration angle (°) | 0.94 | 142.43 ± 39.25 | 109.68 ± 26.03 | 124.42 ± 36.18 | 0.003 ∗ |
| Crown length of impacted tooth (mm) | 0.78 | 11.08 ± 1.02 | 10.90 ± 0.66 | 11.01 ± 0.84 | 0.530 |
| Crown length of homonym tooth (mm) | 0.78 | 11.29 ± 0.86 | 11.05 ± 0.95 | 11.19 ± 0.92 | 0.418 |
| Root length of impacted tooth (mm) | 0.89 | 5.47 ± 1.35 | 7.63 ± 2.00 | 6.66 ± 2.03 | <0.001 ∗ |
| Root length of homonym tooth (mm) | 0.91 | 7.60 ± 1.53 | 10.42 ± 1.95 | 9.15 ± 2.25 | <0.001 ∗ |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


