Chapter 18
Reattachment of permanent incisor enamel fragments
Jane A. Soxman
Indications
Reattachment of an intact enamel fragment for both uncomplicated and complicated crown fracture provides a restoration that is less expensive, rapid, and esthetic with an identical match in original shape, occlusal alignment, natural translucency, surface finish, and unique coloration. This is considered to be interim treatment that does not preclude any future treatment, as no tooth structure is removed or modified. Fracture of permanent incisors is more likely to occur with incompetent lip posture and significant overjet (Bauss et al., 2008; Schatz et al., 2013). Anticipatory guidance is recommended to prepare the patient and parents/guardian for this event (Figure 18.1).

Figure 18.1 Incompetent lip posture with significant overjet.
After an incisor fracture, the enamel fragment should be immediately located and stored in water or a damp paper towel to avoid desiccation, resulting in an opaque appearance and poor bonding (Sharmin & Thomas, 2013) (Figure 18.2). If a lip laceration has simultaneously occurred, the laceration should first be explored for the fragment (Figure 18.3). A lower occlusal radiograph may be obtained to rule out presence of the fragment in the lip.

Figure 18.2 Enamel fragment.
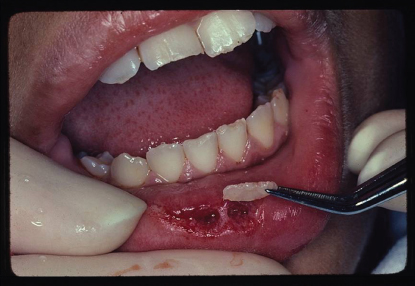
Figure 18.3 Enamel fragment being removed from lower lip laceration.
Procedure
Occlusal, periapical, and eccentric shift shots of the fractured incisor may be obtained to evaluate for root fracture or displacement. The use of local anesthesia should not be necessary for reattachment. The fragment may be reattached with both uncomplicated and complicated fractures. If the fracture has resulted in a borderline pulp exposure, a pulp capping agent, such as calcium hydroxide compounds or white mineral trioxide aggregate (MTA), should be applied, followed by glass ionomer before bonding. A pulpal exposure with a complicated fracture, seen within hours of the exposure and where complete hemostasis is achieved, may be treated conservatively with pulp capping. However, partial pulpotomy generally improves prognosis. If complete hemostasis cannot be achieved or more time has passed, a partial pulpotomy should be performed before reattachment.
If pulp capping with calcium hydroxide followed by glass ionomer is performed, bonding the fragment may no longer be possible due to the layers of material on the incisor now impeding the “fit” between the fragment and incisor. A trough could be prepped in the fragment to accommodate the capping agent and glass ionomer, but the reattachment is compromised. Ultimately, in this case, a composite restoration will most likely be required.
Successful reattachment using only a bonding agent has been reported (Martos et al., 2012; Giudice et al., 2012). Andreasen et al. (1993) reported that reattachment with a bonding resin provides only half the original strength of the intact tooth. Bonding with flowable composite and composite resin has been successfully performed, providing from 2–7 years of function.
A fracture sloping to the cervical enhances the bond with increased area for bonding (Figure 18.4
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


