(1)
Department of Endodontics, New York University College of Dentistry, New York, NY, USA
Abstract
This chapter presents a revision of diagnostic terminology developed by the American Association of Endodontists and indicates both the previous and most current terms and definitions. The clarification is useful to the practitioner as dentists and publications often use different terms to describe pulp/periapical pathosis. This can lead to misunderstandings and confusion. Each diagnostic category is described and its clinical significance is reviewed.
In this chapter, the significance of the term “neuroplasticity” and its relationship to varied painful conditions is elaborated. The term, “atypical odontalgia,” is being revised by the Orofacial Pain Special Interest Group of the International Association for the Study of Pain. The new term, which is more specific, will be “chronic continuous dentoalveolar pain” (CCDAP). This chapter reviews the diagnostic challenge presented by atypical odontalgia (CCDAP).
A self-assessment section provides the reader with an opportunity to evaluate their skills in reaching a diagnosis and treatment plan in challenging cases.
4.1 Synthesis of Information
The final pulpal and periapical diagnosis is based on a synthesis of information collected from the patient’s history of the chief complaint, dental and medical histories, radiographs, sensibility, and clinical tests. The process is challenging since no single test can be considered definitive.
The clinician should have a keen ear capable of interpreting subtle clues in the patient’s narrative and be able to put the clues together with other diagnostic information. At the same time, the clinician must recognize false leads that can result in misdiagnosis and treating the wrong tooth or providing treatment that is not necessary. Tests provide information, but the critical part of the diagnostic process is the ability of the clinician to synthesize information into a rational meaningful complete picture.
4.2 Terminology
There is more than one set of terms used to describe pulp and periapical pathosis. Terminology varies among different organizations to describe the pulp and periapical tissues. Variation in terminology can cause confusion during communication with other dentists (as can different dental numbering systems).
It must be understood that inflamed pulp tissue is in a dynamic state and may have more than one condition existing in the tissue at the same time. For example, underlying deep caries there may be an area of acute inflammation adjacent to chronic inflammation and/or necrosis all of which is in flux. These states may coexist asymptomatically for a long period of time or degenerate rapidly to total necrosis with or without pain. It has been clearly demonstrated that clinical symptoms do not correlate well with histologic findings [7, 9].
The dynamic state of the tissue can produce confusing results during sensibility testing. For example, a root canal may contain necrotic tissue but still have some neural tissue capable of conducting an impulse. In such cases a positive response to testing with cold or electric could mislead the clinician into a diagnosis of a normal responsive pulp. Similarly in a multi-rooted tooth, one root may contain responsive pulp tissue, while the other is completely necrotic. In that case, pulp testing would not indicate the presence of pulp necrosis.
The American Association of Endodontists (AAE) recently published (2012) a revised list of pulp and periapical diagnostic terms and definitions (Table 4.1). The terminology is useful in categorizing cases and their treatment. There are other pulp classifications, but the AAE provides the most recent revision available. There is no universal agreement concerning the validity of this terminology.
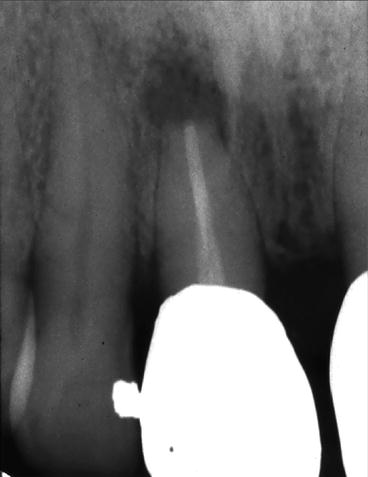
Fig. 4.1
Failing root canal therapy. Following emergency treatment, the case will be retreated and followed to determine if apical surgery is required. Footnote: This radiograph demonstrates previously treated tooth #8. Please note the periapical lesion and apical resorption. The patient presented in severe pain, without swelling, isolated to #8. Following emergency treatment, non-surgical root canal therapy will be redone. The patient will be followed to determine the need for apical surgery
Table 4.1
A 2012 revision of terminology by the American Association of Endodontists indicates both the previous and most current terms and definitions
|
Old term
|
New term
|
Definition
|
|---|---|---|
|
Normal pulp
|
Normal pulp
|
A clinical diagnostic category in which the pulp is symptom-free and normally responsive to pulp testing
|
|
Reversible pulpitis
|
Reversible pulpitis
|
A clinical diagnosis based upon subjective and objective findings indicating that the inflammation should resolve and the pulp return to normal
|
|
Irreversible pulpitis
|
Symptomatic irreversible pulpitis
|
A clinical diagnosis based on subjective and objective findings indicating that the vital inflamed pulp is incapable of healing. Additional descriptors: lingering thermal pain, spontaneous pain, referred pain
|
|
Asymptomatic irreversible pulpitis
|
A clinical diagnosis based on subjective and objective findings indicating that the vital inflamed pulp is incapable of healing. Additional descriptors: no clinical symptoms but inflammation produced by caries, caries excavation, trauma, etc.
|
|
|
Pulp necrosis
|
Pulp necrosis
|
A clinical diagnostic category indicating death of the dental pulp. The pulp is usually nonresponsive to pulp testing
|
|
Previously treated (pulpless)
|
Previously treated
|
A clinical diagnostic category indicating that the tooth has been endodontically treated and the canals are obturated with various filling materials other than intra-canal medicaments
|
|
Normal periapical (periradicular) tissues
|
Normal apical tissues
|
Teeth with normal periradicular tissues that is not sensitive to percussion or palpation testing. The lamina dura surrounding the root is intact, and the periodontal ligament space is uniform
|
|
Acute periapical (periradicular) periodontitis or chronic apical (periradicular) periodontitis with symptoms
|
Symptomatic apical periodontitis
|
Inflammation, usually of the apical periodontium, producing clinical symptoms including a painful response to biting and/or percussion or palpation. It may or may not be associated with an apical radiolucent area
|
|
Chronic periapical (periradicular) abscess periodontitis
|
Asymptomatic apical periodontitis
|
Inflammation and destruction of apical periodontium that is of pulpal origin appears as an apical radiolucent area and does not produce clinical symptoms
|
|
Acute apical (periradicular) abscess
|
Acute apical abscess
|
An inflammatory reaction to pulpal infection and necrosis characterized by rapid onset, spontaneous pain, extreme tenderness of the tooth to pressure, pus formation, and swelling of associated tissues
|
|
Chronic apical (periradicular) abscess or phoenix abscess or suppurative apical periodontitis
|
Chronic apical abscess
|
An inflammatory reaction to pulpal infection and necrosis characterized by gradual onset, little or no discomfort, and the intermittent discharge of pus through an associated sinus tract
|
|
Focal sclerosing osteomyelitis
|
Condensing osteitis
|
Diffuse radiopaque lesion representing a localized bony reaction to a low-grade inflammatory stimulus, usually seen at apex of the tooth
|
4.3 Neuroplasticity
A major development in the field of pain physiology was the discovery of neuroplasticity in the late twentieth century. According to this concept, experiences like thinking, learning, and habits (addiction) can significantly change both the brain’s physical structure (anatomy) and its functional organization (physiology). Neuroplasticity has an obvious positive side, including all forms of learning and adaptive responses to injury or other personal experiences. However, it also can have a destructive effect due to negative experiences [3].
Neuroplasticity may explain expanded areas of patients’ perception of pain beyond what might be expected (i.e., the area of the body feeling pain is more extensive than that which was actually injured) or as chronic pain (i.e., the original injury or disease has resolved, but the pain remains and may even increase). Both of these are examples of a negative manifestation of neuroplasticity, which explains many previously misunderstood phenomena but also poses a significant management challenge for pain therapists and dentists. All dentists and physicians should appreciate the implications of neuroplasticity since it helps understanding their patients’ complaints of pain [3].
“Neuroplasticity” is a term that describes how the nervous system changes in response to painful and other stimuli. To understand this process, it is important to recognize that the simple model of a painful stimulus leading to a proportional response has been replaced by a much more complex model of nervous system behavior.
The following sections will amplify each of the diagnostic terms.
4.4 Reversible Pulpitis
This highly subjective term is based on the history of the chief complaint as well as information drawn from radiographs and sensibility tests. A reversible pulpitis must be seen in the context of tissue in a dynamic state. There is no single diagnostic test that provides defining data about the exact histologic state of the pulp or its prognosis. The clinician must synthesize all available data including history of the pain, its severity, and the treatment plan. The patient’s narrative is extremely important.
Important questions for the patient include:
-
When did the pain start?
-
Did it follow a new restoration or occur spontaneously?
-
What makes the tooth hurt?
-
What makes the pain stop?
-
Did the pain start suddenly after biting on something hard?
-
Is the pain getting worse?
-
Does it wake you up at night?
-
Can you chew on the tooth without pain?
-
What medication are you using for pain? Is it effective?
-
On a scale of 1–10 with 1 being very mild and 10 being unbearable, how would you rank your pain?
Radiographic findings may include the presence of decay, old pulp caps, large restorations, periodontal disease, all of which add to the picture. The patient’s response to the above questions, combined with diagnostic findings point the way to determining if the diagnosis is of odontogenic or non-odontogenic origin. It helps to clarify if there is reversible pulpitis, not requiring intervention, or requires treatment.
The clinician should explain his diagnosis and treatment plan to the patient and note that additional follow-up may be required.
4.5 Cold Sensitivity Following a Restorative Procedure
A complaint of cold sensitivity after an operative procedure requires follow-up to determine if the symptom of cold sensitivity disappears, remains the same, or gets worse over days, weeks, or months. A particularly difficult question occurs when there is a persistent moderate level of pain that neither progresses toward less pain nor does not increase in severity. Clearly, there is a time period beyond which it is not reasonable to wait any longer to make a decision about treatment from patient to patient. There is no simple answer to the question of how long to wait, and the variables include patient’s dental history, severity of pain, and the ultimate treatment plan.
For example, if the tooth in question is to be restored with a crown, there should be no question about the status of the pulp when the restoration is completed and ready to be cemented. If moderate pain persists over a number of weeks or there is an inability to use the tooth during function, it becomes increasingly clear that endodontic therapy is necessary.
At no time should the patient be pushed into treatment that he/she does not fully understand or desire. In cases where there is severe pain that suddenly disappears, it is advisable to apply sensibility tests again in order to determine if the absence of pain is due to healing or devitalization.
Clinical Tips
-
Do not place a final restoration until the status of the pulp is resolved.
-
Root canal therapy cannot “always be done later,” without damaging the restoration. For example, consider the difference between treating a mandibular incisor with or without a crown present. The narrowness of the prepared tooth under the crown would make access difficult and probably result in damage to the integrity of the crown.
4.6 Symptomatic Irreversible Pulpitis
This diagnosis is based on subjective and objective findings that lead to a conclusion that the pulp in question does not have the capacity to heal. Important factors to consider include the presumed cause of the pain, its severity and duration, as well as the patient’s ability to use it during function.
For example, a large pulp exposure due to caries or a traumatic fracture represents serious problems that would not be considered reversible. In contrast, pain sensitivity following a crown preparation may not be immediately recognized as reversible or irreversible. Severe lingering pain after the application of cold or heat sensitivity is taken as a classic sign of irreversible pulpitis. Irreversible pulpitis can be treated by endodontic therapy or extraction.
Clinical Tips
When treating a tooth with irreversible pulpitis:
-
Teeth with irreversible pulpitis often pose a challenge in achieving complete dental anesthesia. It is beneficial to test a tooth with cold, heat, or percussion (the chief complaint) rather than just depending on a numb lip to be an indicator of successful anesthesia.
-
Be prepared to utilize alternative anesthetic techniques including intraosseous, ligamental, and intrapulpal injections.
-
If time does not permit complete instrumentation of a canal(s), pulpotomy (all tissue from the chamber is removed but canal(s) is not entered) has been shown to be an effective means of reducing pain.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


