Fig. 22.1
(a, b) Protraction of the maxillary complex using orthopedic forces. The maxilla articulates with nine bones: two of the cranium, the frontal and ethmoid, and seven of the face, viz., the nasal zygomatic, lacrimal, inferior and nasal concha, palatine, vomer, and its fellow of the opposite side. Sometimes it articulates with the orbital surface and sometimes with the lateral pterygoid plate of the sphenoid. Illustration showing how protraction forces applied to the maxilla depends on the disarticulation and growth at all the dependent sutures (Courtesy of E. Genevoc)
Some of the earlier work in this field, which encouraged a rethinking of the use of orthopedic forces for the correction of midfacial retrusion, includes Hass (1970), Delaire (1971), Delaire et al. (1972, 1973, 1976, 1978), Irie and Nakamura (1974), Ranta (1988), Subtelny (1980), Friede and Lennartsson (1981), Sarnas and Rune (1987), Berkowitz (1982), Tindlund (1989), Nanda (1978), and Molstad and Dahl (1987). More recently, this area has been influenced by the work of Tindlund et al. (Irie and Nakamura 1974; Ranta 1988; Subtelny 1980; Delaire et al. 1978; Friede and Lennartsson 1981; Sarnas and Rune 1987; Berkowitz 1982; Tindlund 1989; Tindlund and Rygh 1993; Nanda 1978; Molstad and Dahl 1987) and Buschang et al. (1994).
Earlier attempts by Kettle and Burnapp (1955) in which anteriorly directed extraoral forces were derived from chin caps were relatively unsuccessful. Facial mask therapy seems to offer better control and a wider range of force application.
In many cases, in the mixed dentition, palatal expansion using fixed orthodontic appliances was applied simultaneously with protraction to correct a bilateral crossbite and create a more favorable condition for midfacial growth and development.
Prior to the use of orthopedic forces, many standard orthodontic treatments designed to move the dentition to correct a class III malocclusion due to midfacial retrusion in the absence of mandibular prognathism failed. Orthodontic forces applied to the teeth by class III elastics would not displace the maxilla; at best, they would flare the maxillary incisors without creating an adequate incisor overbite and axial inclination. This treatment was found to be unsatisfactory and soon fell out of favor.
Since 1975, Berkowitz has been using a modified protraction facial mask originally popularized by Delaire et al. (1972) (Figs. 22.2, 22.3, and 22.4). It has been very successful in controlling the direction of protruding forces without causing severe sore spots on the chin or forehead. He has found that protraction forces do not modify the direction of mandibular growth as Delaire et al. (1972) claimed, but by increasing midfacial height, the mandible is repositioned downward and backward with growth to make the patient’s maxillary retrusion appear less evident.
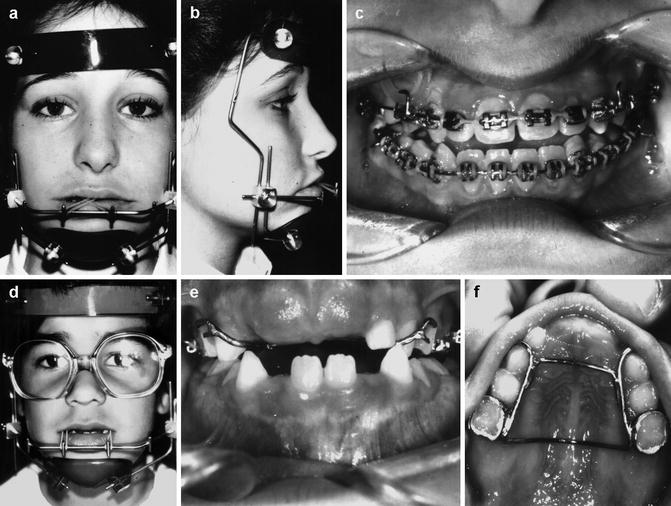
Fig. 22.2
(a) Frontal and (b) lateral views of a Delaire-style protraction facial mask. Padded chin and forehead rests distribute reaction forces of 350–400 g per side equally to both areas. Elastics are attached to hooks placed on the arch wire between the cuspids and lateral incisor. (c) Intraoral view of edgewise rectangular arch with hooks for protraction elastics. (d–f) Delaire-style protraction facial mask used with a fixed labial-palatal wire framework. Elastic forces of 350–400 g per side can still be used with this intraoral framework
Fig. 22.3
(a–x) Case BB (WW-62). Maxillary protraction in a UCLP. (a) Complete unilateral cleft lip and palate. (b, c) Lip and nose after surgery. (d) Cuspid crossbite of the lateral cleft segment at 5 years of age due to mesioangular rotation of the palatal segment. (e) Buccal occlusion after expansion using a quad helix expander. (f, g) 6 years of age. Note relapse of cuspid crossbite due to failure of using a palatal arch retainer. (h) Palatal view showing good arch form (i, j) Facial photographs at 8 years. (k) Orthodontic alignment of incisors prior to secondary alveolar bone graft. (l) Protraction facial mask with elastics. (m, n) class III elastics used to maintain tension at circumaxillary suture during the time not wearing protraction forces. (o) Occlusion after orthopedic–orthodontic forces. Lateral incisor space regained. (p) Removal retainer with lateral incisor pontic (q, r) Fixed bridge at 18 years of age replacing missing lateral incisor and stabilizing maxillary arch form. (s–u) 17 years prior to nose–lip revision. (v–x) Facial photos at 19 years, showing good facial symmetry after revision
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


