Create Symmetry
All patients with malocclusions present with some asymmetries, both skeletal and dental. The simplest and best method to correct these problems is to apply symmetric forces to the teeth and jaws. This statement is based solely on the results of my clinical experience. To my knowledge, this issue has not been addressed in the clinical literature. In a future volume of this series, an entire chapter will be devoted to the treatment of major asymmetries that require more complex treatment plans, such as asymmetrical extractions or surgery, which usually occur in adult patients.
When treating growing patients, however, the skeletal and dentoalveolar response to various orthodontic and orthopedic forces will routinely produce symmetric, esthetically pleasing, stable results.
Rationale for Starting Treatment in the Maxilla
After having been taught to begin treatment in the mandibular arch, I experimented with banding the maxillary arch first. This change in treatment procedure, in which the maxillary arch was treated before the mandibular arch, came as a result of the following observations:
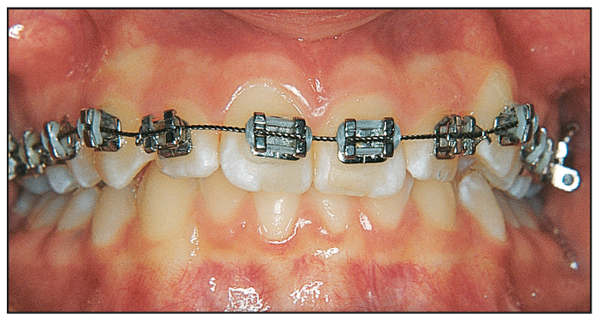
- If the maxillary arch is treated first, the bite opens, and the mandibular curve of Spee begins to level, making it simpler to band and bond the mandibular arch later (Figs 15-1 and 15-2).
- Because there are fewer opposing occlusal forces, the mandibular arch routinely is corrected faster.
- Because it is no longer restricted by the occlusion, the mandible may begin to grow, making the facebow more effective.
- Maxillary incisors face less occlusal interference from mandibular anterior brackets because the occlusion has opened.
- The patient experiences less discomfort because the arches are not treated simultaneously.
- Patients and parents are happier when maxillary brackets are placed first so that they can “show off” their new braces.

It is therefore preferable to treat the maxilla first and create an ideal maxillary arch, even though it is in an asymmetric environment.
Facebow is more effective when the maxillary arch is treated first because the occlusion is changed and interferences removed, thereby unlocking the mandible and allowing it to better express its potential growth. In addition, the orthopedic effect of the facebow on the tied-back maxillary archwire holds the maxilla in position while the mandible grows downward and forward. In patients with severe deep bite, a bite plate (removable retainer), Guray Bite Raisers (GAC), or bonded lingual brackets (Bite Turbos, Ormco) can be used to facilitate this process.
When moderate asymmetries are present in the original malocclusion, first establishing symmetry in the maxillary arch prompts the mandible to respond toward greater symmetry without special treatment. The following three hypotheses may explain this effect:
- If the maxillary arch is treated first, the therapy will simulate a splint effect by moving these teeth out of their original occlusion, thereby allowing the mandibular occlusion to be unlocked from asymmetric occlusal forces. This will allow the mandible to “relax” and grow into better symmetry. Centric relation shifts often are resolved with bracketing of the maxillary arch.
- When facebow is used in a patient with a Class II subdivision malocclusion, although the occlusion is asymmetric, the symmetric design of the facebow (Fig 15-3) will apply more force to the Class II side, thus encouraging correction on that side. The asymmetric molar positions will make the symmetric facebow fit asymmetrically, thereby causing the outer bow on the Class II side to be positioned more outwardly. This will increase the force on the Class II side.
- An asymmetric force is definitely being applied to the side of the face if the patient sleeps on one side. If this posture is repeated over many months, it is feasible that it could affect the patient’s growth pattern and make it more asymmetric. The outer bows of the facebow compel the patient to sleep on his or her back instead of the side of the face, which can encourage or allow symmetric growth of the mandible (Fig 15-4).

In addition to the facebow, the lip bumper is also symmetrically designed (Fig 15-5) and can provide similar forces. If the patient sleeps on his or her side, the lip bumper wire can irritate the inside of that cheek.
Treatment Sequence
Arch coordination
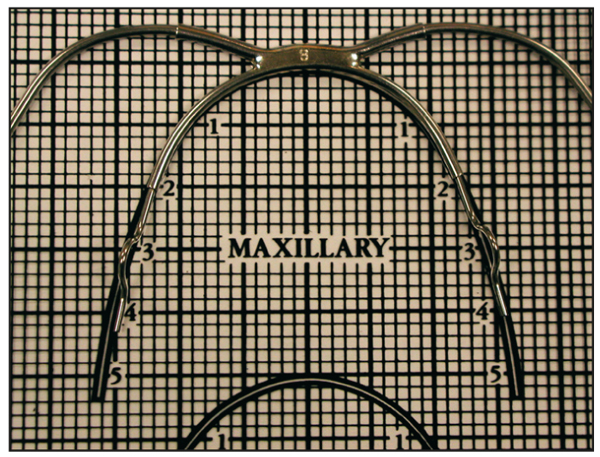
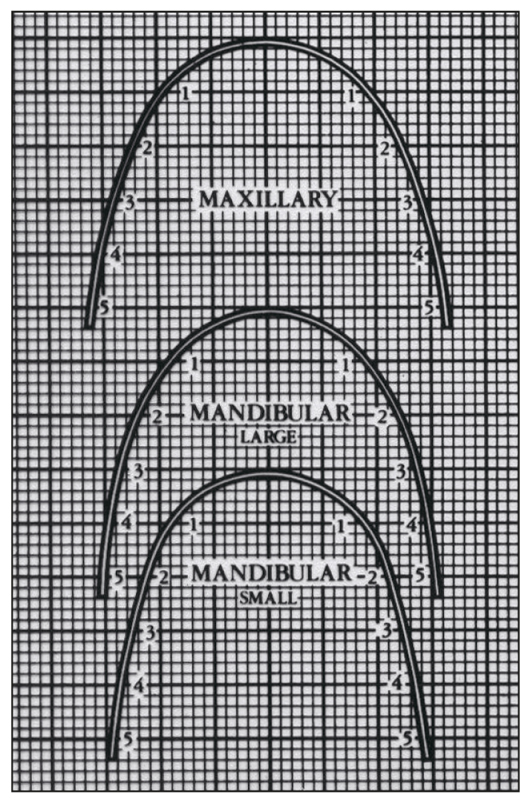
As detailed in principle 9 on arch form, coordination of arches is essential to create occlusal symmetry. Maintaining the original mandibular intercanine width is critical to stability. The Alexander preformed archwire template is effective in coordinating the maxillary and mandibular anterior canine-to-canine relationships, thus maintaining intercanine width (Fig 15-6).
Almost every Class II malocclusion requires maxillary canine, premolar, and molar expansion, but it is necessary to determine the amount of expansion required. A simple procedure to answer this question is to ask the patient to protrude the mandible forward until the incisor teeth are almost edge to edge and then observe how much maxillary posterior overjet expansion would be needed to bring these teeth into good relationship with the untreated mandibular posterior teeth.
The maxillary arch form is then created to coordinate with the anticipated Class I relationship of the currently untreated mandibular arch. This archwire is shaped in an ideal arch form.
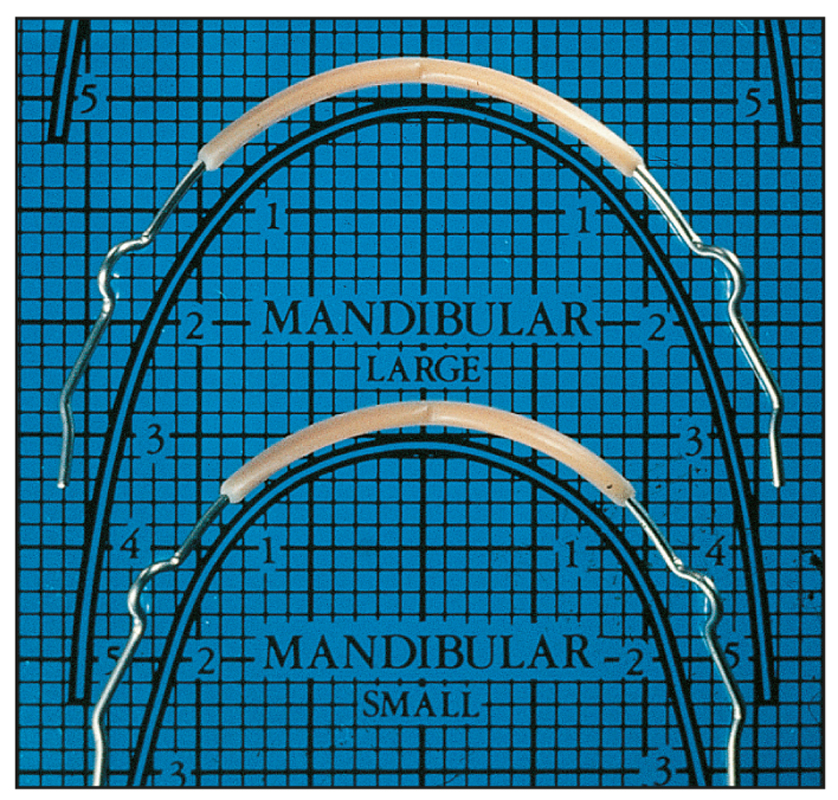
Likewise, when the final ideal mandibular arch form is established, the original intercanine width is maintained and the posterior region shaped to coordinate with the treated maxillary arch form. If this procedure is followed, the final results will be coordinated archwires (Fig 15-7) reflecting normal and stable buccal overjet. Only rarely will it be necessary to coordinate both archwires by removing and replacing them, a/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


