This case report describes the orthodontic treatment of an 11-year-old girl with solitary median maxillary central incisor syndrome, a presumed microform of holoprosencephaly. Because both second premolars were missing in the maxilla, deciduous molar extraction and orthodontic space opening were performed, moving the solitary median maxillary central incisor electively off-center. A mandibular second premolar was transplanted to replace the missing incisor. The resulting spaces could be orthodontically closed in both arches. Prosthodontic reshaping of the transplanted tooth after debonding completed the dental treatment.
Highlights
- •
A single upper central incisor without trauma history might be a predictor of holoprosencephaly.
- •
Tooth transplantation is considered an advantageous treatment to replace a maxillary incisor.
- •
Orthodontic treatment of adolescents with SMMCI syndrome can be performed successfully.
Solitary median maxillary central incisor (SMMCI) syndrome was first introduced by Hall et al in 1997, describing a developmental abnormality with an uncertain etiology. An incidence of 1 in 50,000 live births was estimated. The characteristic and most prominent trait of this condition is the single incisor that develops and erupts precisely in the midline of the maxillary dental arch in both the deciduous and permanent dentitions. The crown morphology of the SMMCI is strictly symmetric. Further oral features are a pseudonotched or arch-shaped appearance of the upper lip with an indistinct philtrum, the absence of a labial frenulum, and a V-shaped palate with an unusual narrow ridge along the midpalatal suture. According to Kjaer et al, SMMCI syndrome is the mildest form of holoprosencephaly, a developmental defect affecting the forebrain, with cyclopia as its most severe expression. The spectrum of associated anomalies shows wide variability; however, the following features were found to be typical of the syndrome: preterm birth and low birth weight in 37% of cases, potentially life-threatening congenital nasal airway obstruction (choanal atresia, midnasal stenosis, or nasal pyriform aperture stenosis in over 90%), short stature in 50%, small head circumference in 33%, hypotelorism in 45%, intellectual disability varying in degree in 50% (from slow learning to intellectual retardation), possible association with epilepsy and attention-deficit/hyperactivity disorder, and deviant sella turcica and pituitary gland morphologies.
Regarding comprehensive orthodontic treatment in patients with SMMCI syndrome, there are only 2 reports in the literature: Bolan et al described rapid maxillary expansion in a 6-year-old boy monitored with cone-beam computed tomography. Although his posterior crossbite could be clinically corrected, the tomography showed no opening of the midpalatal suture because of probable fusion of the anterior sutural region, where the SMMCI is typically located. Lygidakis et al reported on a 14-year follow-up of a male patient with SMMCI syndrome. After maxillary expansion at the age of 4, anterior space was created orthodontically to insert a Maryland bridge for replacement of the missing central incisor at the age of 16.
This report concentrates on the orthodontic management of a patient with SMMCI syndrome and promotes premolar transplantation as an advantageous treatment approach.
Diagnosis
An 11-year-old girl presented with a single maxillary central incisor at the orthodontic department of the Medical University of Vienna in Austria. Her parents requested a second opinion concerning orthodontic treatment. After having made records alio loco, both the panoramic and the lateral skull radiographs were already available. Allergies to pollen, animal hair, and penicillin were reported. There was no family history of hereditary disease. The patient’s medical history indicated respiratory distress and surgery soon after birth. Neither the surgeon nor the pediatrician could be contacted for details. However, narrowing of her nasal airways persisted to some extent, resulting in habitual mouth breathing. Bruxing was reported by the parents, causing the first signs of dental wear on the mandibular incisors. Neither temporomandibular joint problems nor a centric relation-centric occlusion discrepancy was found.
The clinical examination showed a dolichocephalic, symmetric face with harmonious facial thirds and a narrow nose ( Fig 1 ). The profile was convex with a decreased nasolabial angle and a retrognathic chin. A high central portion of the upper lip with an indistinct philtrum was the extraoral characteristic of the SMMCI syndrome. The maxillary central incisor was positioned precisely in the facial midline.

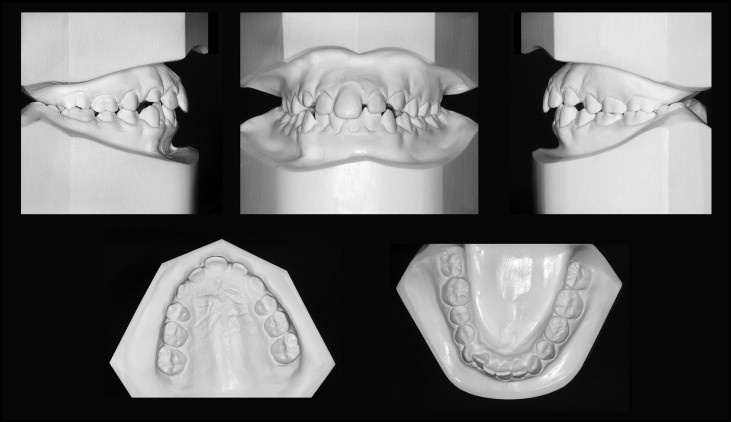
Intraorally, the patient was in the late mixed dentition with 3 remaining second deciduous molars ( Fig 2 ). A surplus of space could be detected in both arches (1 mm in the mandibular arch considering leeway space, 3.9 mm in the maxillary arch). There were both a Class I molar relationship on the left side and a Class II tendency (a quarter unit) on the right side. Overjet accounted for 3 mm, and overbite for 4 mm. The mandibular dental midline was shifted 1 mm to the right. The typical intraoral features of SMMCI syndrome were a V-shaped palate with a marked midpalatal vomerine ridge, the absence of the labial frenulum of the upper lip, and the symmetric crown form of the SMMCI with normal crown dimensions. The contour of both approximal surfaces of this incisor had the characteristic anatomic shape of the distal surface of a normal central incisor.
In addition to the absence of a maxillary central incisor, the panoramic radiograph showed agenesis of both maxillary second premolars ( Fig 3 ). The corresponding deciduous molars were still present. The left second deciduous molar was also persistent in the mandible, indicating an asymmetric tooth eruption pattern of the mandibular second premolars. The maxillary second molars were about to erupt. The germs of the mandibular third molars could be identified. No caries lesions or fillings were detectable. The narrow nasal cavity with a slight asymmetric nasal septum was characteristic of SMMCI syndrome.

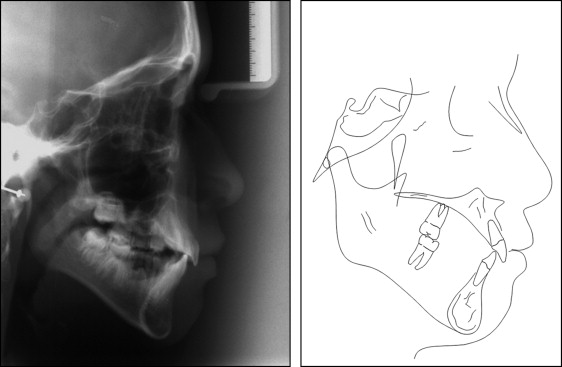
The cephalometric data indicated a considerably vertical Class I relationship with a vertical jaw relationship: ANS-PNS/Go-Gn, 31° ( Fig 4 ). Both jaws were retrognathic (SNA angle, 79°; SNB angle, 76°) and posteriorly inclined (S-N/ANS-PNS, 10°; S-N/Go-Gn, 41°). Dental and dento-basal relationship measurements showed average values. The morphology of the pituitary fossa appeared to be normal.
In terms of other syndrome-associated anomalies, the patient had no intellectual disability and showed no hypotelorism. She had a slightly shorter stature than her 1-year-younger sister.
Treatment objectives
The treatment goals included orthodontic space opening in the maxillary incisor region and autogenous transplantation of a mandibular second premolar, consecutively. Space closure would be performed in the donor tooth region as well as in the maxilla, where the second premolars were missing, achieving a Class II molar relationship on the right side and a Class I relationship on the left side. Finally, recontouring of the maxillary incisors was planned.
Since the SMMCI did not have the morphology of a right or left central incisor, orthodontic space opening would be performed on the left, where more space was initially available. Thus, the recipient site for the transplant was determined to be the left central incisor region.
Treatment objectives
The treatment goals included orthodontic space opening in the maxillary incisor region and autogenous transplantation of a mandibular second premolar, consecutively. Space closure would be performed in the donor tooth region as well as in the maxilla, where the second premolars were missing, achieving a Class II molar relationship on the right side and a Class I relationship on the left side. Finally, recontouring of the maxillary incisors was planned.
Since the SMMCI did not have the morphology of a right or left central incisor, orthodontic space opening would be performed on the left, where more space was initially available. Thus, the recipient site for the transplant was determined to be the left central incisor region.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


