Auricular deformities, particular prominent ears, are a common congenital anomaly affecting nearly 5% of the white population. Children with auricular deformities are likely to experience ridicule by their peers. Prominent ears, commonly referred to as prominauris, can be predictably treated before children enter school, thus avoiding the emotional trauma caused by ridicule. Whereas cosmetic surgery is performed primarily in the adult population, otoplastic surgery is performed primarily on children and can be an invaluable service for the patient and satisfying for the surgeon.
Numerous publications have described the correction of auricular deformities. The surgeon must understand the history of these various techniques to develop a predictable and successful method of addressing the problem of prominent ears. Dieffenbach is credited with the first otoplastic technique to correct a prominent auricle in 1885. Ely, in 1881, authored the first case report describing correction of prominent ears in a 12-year-old boy who was being teased at school. Since that report, more than 170 surgical techniques have been described in the literature for the correction of prominent ears.
When clinically evaluating the facial complex, the ears often are overlooked. If protruding ears are present, reduction otoplasty as an adjunctive or isolated procedure can be predictably performed, often with satisfying results. A thorough understanding of the embryology and development of the human auricle, along with the resultant external anatomy of the ear, is of paramount importance in developing a reliable technique to deal with common auricular deformities.
EMBRYOLOGY OF THE AURICLE
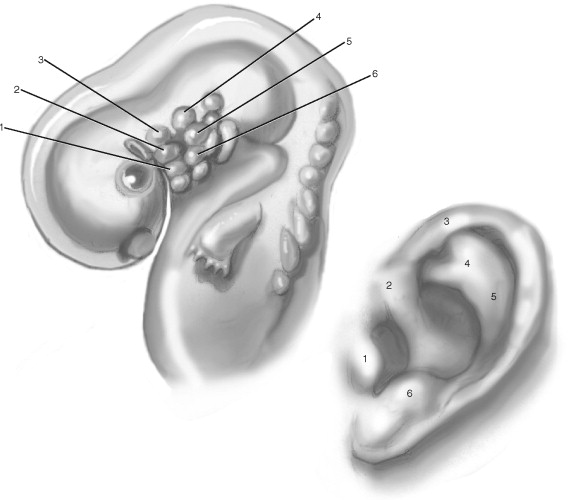
Malformations of the auricle are common, occurring in 1 in 12,500 births. They can occur alone or in combination with a syndrome affecting the head and neck structures. The embryogenesis of the auricle exemplifies in miniature the precise and logical progressions characteristic of the developing human form. The external ear development during the third to twelfth weeks of embryonic life is complex. The precursors to the auricle present from days 36 to 38 of intrauterine life, developing first from the first branchial groove where the first (mandibular) and second (hyoid) branchial arches are present ( Figure 32-1 ). Both arches give rise to the auricular hillocks, often referred to as the auricular tubercles of His. Hillock numbers 1, 2, and 3 arise from the caudal border of the mandibular arch, and numbers 4, 5, and 6 are formed from the cephalic border of the hyoid arch. The auricular hillocks present in their most prominent and characteristic form by intrauterine day 41. During this same stage, the groove between the mandibular and hyoid arches (hyomandibular groove) widens and deepens by the increased growth of the hillocks. This groove eventually forms the external auditory canal and concha. By days 43 to 45, the hillocks have migrated and coalesced to form the auricle. During this union the mesenchyma of the hyoid arch increases substantially relative to the mandibular arch to contribute 85% of the external adult ear. Hillocks 2 and 3 from the mandibular arch lose their individuality and fuse to form the helical crus. Later, hillocks 4 and 5 from the hyoid arch merge and alter their configuration as they give rise to the helix and antihelical fold. Hillock 1 remains prominent and becomes the tragus, and hillock 6 becomes the antitragus.
SURGICAL ANATOMY
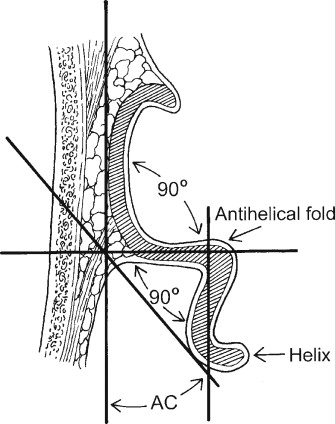
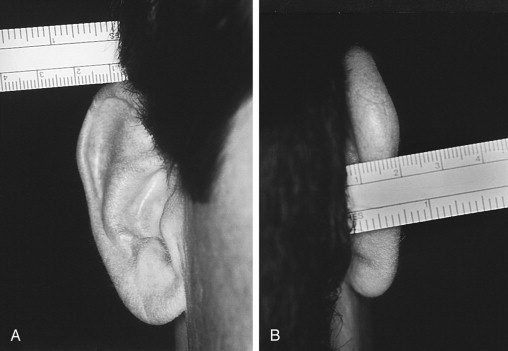
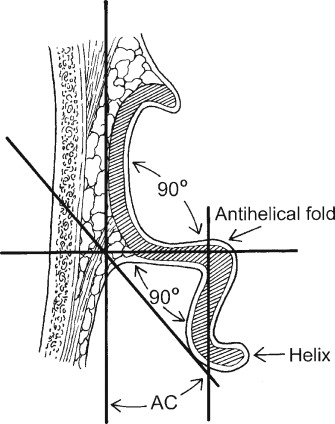
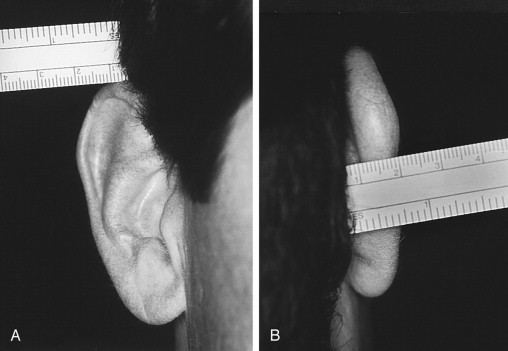
The majority of the growth of the pinna is completed by an early age. The average child has 85% of ear development completed by age 3 years. The ear is nearly fully grown by the age of 7 to 8 years. Ear height continues to grow into adulthood, but the width and distance of the ear from the scalp change little after 10 years of age. Of note, a person’s two ears often vary in size and shape from each other. The average adult ear is approximately 6.5 cm in length and 3.5 cm in width. In the “normal” ear, the auricle lies between horizontal lines drawn from the upper rim of the orbit and the nasal spine. The normal posterior wall of the conchal bowl is set at an angle of approximately 90 degrees to the mastoid. A second 90-degree angle is formed at the antihelical fold and is called the scapha-conchal angle. These two angles, in combination with the curvature of the helix, set the auricle adjacent to the scalp at approximately 25 to 35 degrees, forming the auriculocephalic angle ( Figure 32-2 ). When correcting prominent ears, three important anatomic “pearls” can be used intraoperatively to assess the final result: (1) the helical rim should be seen just lateral to the most lateral presence of the antihelix from the frontal view; (2) the distance measured between the helical rim and the mastoid area is slightly less than 2 cm; and (3) the distance between the skull and the uppermost aspect of the helix is approximately 1 cm ( Figure 32-3 ).
The auricular cartilage is a unique, intricately shaped, and delicate structure with multiple elevations and depressions that provide both skeletal support and form to the adult ear. The cartilage of the auricle is a single piece of yellow (elastic) fi brocartilage with a complicated relief on the anterior, concave side and a smooth, posterior, convex side. Cartilage thickness is fairly uniform throughout. The cartilage is covered on both surfaces by a thin, firm, adherent layer of perichondrium. The anterior lateral surface of the cartilage is covered with fine, thin skin, closely adherent to the cartilaginous framework. Subcutaneous fat is practically nonexistent, but a diffuse subdermal vascular plane exists that supports flap viability. The posterior surface of the cartilage framework is draped with less-adherent skin that contains two layers of fat and a larger subdermal plexus of arteries, veins, and nerves.
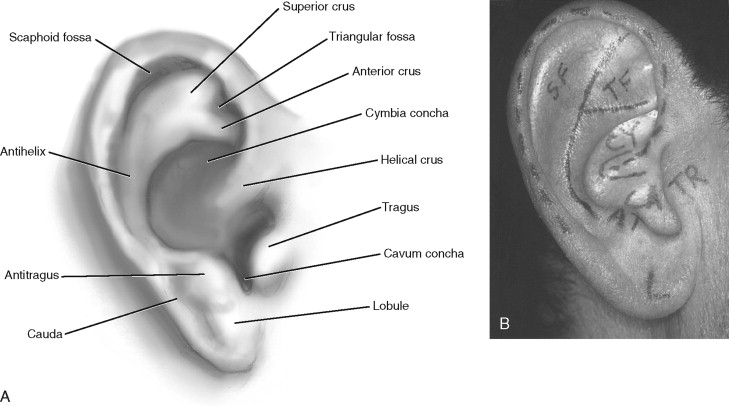
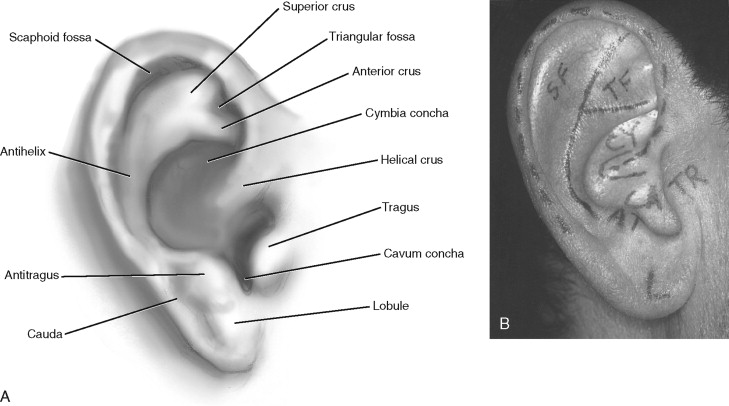
A helical border terminates anteriorly in a crus that lies almost horizontally above the external auditory meatus. The antihelix crowning the posterior conchal separates and diverges into both a superior and an anterior crus enclosing the triangularis fossa. Between the helix and the antihelix lies a long, deep furrow called the scapha. The conchal cavity, composed of the cymba (superior) and cavum (inferior) concha, arises from the floor, which is at least 1 cm deeper than the overlying tragus and antitragus. The inferior tip of the helical cartilage is referred to as the cauda, and extending from this inferiorly is the lobule, which hangs without any skeletal framework ( Figure 32-4 ).
SURGICAL ANATOMY
The majority of the growth of the pinna is completed by an early age. The average child has 85% of ear development completed by age 3 years. The ear is nearly fully grown by the age of 7 to 8 years. Ear height continues to grow into adulthood, but the width and distance of the ear from the scalp change little after 10 years of age. Of note, a person’s two ears often vary in size and shape from each other. The average adult ear is approximately 6.5 cm in length and 3.5 cm in width. In the “normal” ear, the auricle lies between horizontal lines drawn from the upper rim of the orbit and the nasal spine. The normal posterior wall of the conchal bowl is set at an angle of approximately 90 degrees to the mastoid. A second 90-degree angle is formed at the antihelical fold and is called the scapha-conchal angle. These two angles, in combination with the curvature of the helix, set the auricle adjacent to the scalp at approximately 25 to 35 degrees, forming the auriculocephalic angle ( Figure 32-2 ). When correcting prominent ears, three important anatomic “pearls” can be used intraoperatively to assess the final result: (1) the helical rim should be seen just lateral to the most lateral presence of the antihelix from the frontal view; (2) the distance measured between the helical rim and the mastoid area is slightly less than 2 cm; and (3) the distance between the skull and the uppermost aspect of the helix is approximately 1 cm ( Figure 32-3 ).
The auricular cartilage is a unique, intricately shaped, and delicate structure with multiple elevations and depressions that provide both skeletal support and form to the adult ear. The cartilage of the auricle is a single piece of yellow (elastic) fi brocartilage with a complicated relief on the anterior, concave side and a smooth, posterior, convex side. Cartilage thickness is fairly uniform throughout. The cartilage is covered on both surfaces by a thin, firm, adherent layer of perichondrium. The anterior lateral surface of the cartilage is covered with fine, thin skin, closely adherent to the cartilaginous framework. Subcutaneous fat is practically nonexistent, but a diffuse subdermal vascular plane exists that supports flap viability. The posterior surface of the cartilage framework is draped with less-adherent skin that contains two layers of fat and a larger subdermal plexus of arteries, veins, and nerves.
A helical border terminates anteriorly in a crus that lies almost horizontally above the external auditory meatus. The antihelix crowning the posterior conchal separates and diverges into both a superior and an anterior crus enclosing the triangularis fossa. Between the helix and the antihelix lies a long, deep furrow called the scapha. The conchal cavity, composed of the cymba (superior) and cavum (inferior) concha, arises from the floor, which is at least 1 cm deeper than the overlying tragus and antitragus. The inferior tip of the helical cartilage is referred to as the cauda, and extending from this inferiorly is the lobule, which hangs without any skeletal framework ( Figure 32-4 ).
BLOOD SUPPLY
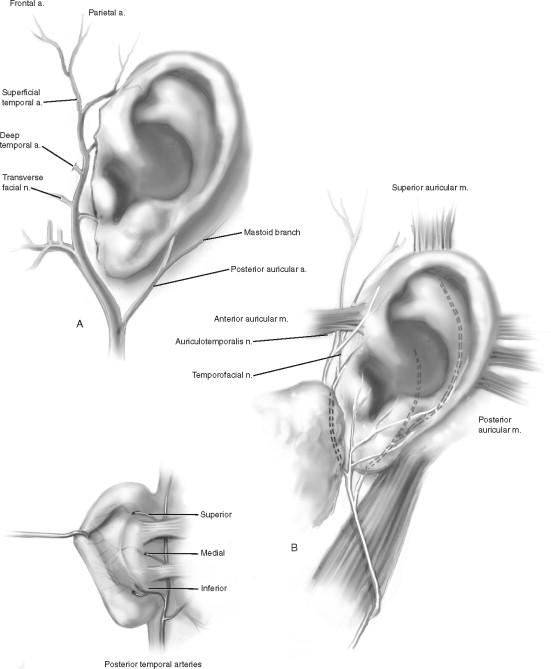
The arterial blood supply to the ear is principally derived from two main branches of the external carotid artery: the superficial temporal artery and the posterior auricular artery. The superficial temporal artery emerges from the parotid capsule 1 cm in front of the ear deep to the veins and below the anterior auricular muscle. It gives off the superior, medial, and inferior branches, supplying the anterior and anterolateral surface of the auricle. The posterior surface is dominantly supplied by the posterior auricular artery, which travels parallel to the postauricular crease upward, crossing below the great auricular nerve and under the posterior auricular muscle. Awareness of this relation is important to avoid damage to the artery or nerve during surgery. The posterior auricular artery gives off three branches—superior, medial, and inferior—that provide a greater volume of blood to the postauricular ear than its anterior counterparts. These same vessels perforate the auricular cartilage over a large surface of the anterior ear and anastomose with the branches of the superficial temporal artery. The external ears have a tremendous blood supply, allowing multiple surgical approaches and salvage of the ear after traumatic avulsion.
Venous drainage of the ear by way of the complementary veins is into the external jugular vein. Lymphatic drainage is into three surrounding areas by way of the complex and extensive network of lymphatic vessels.
NERVE SUPPLY
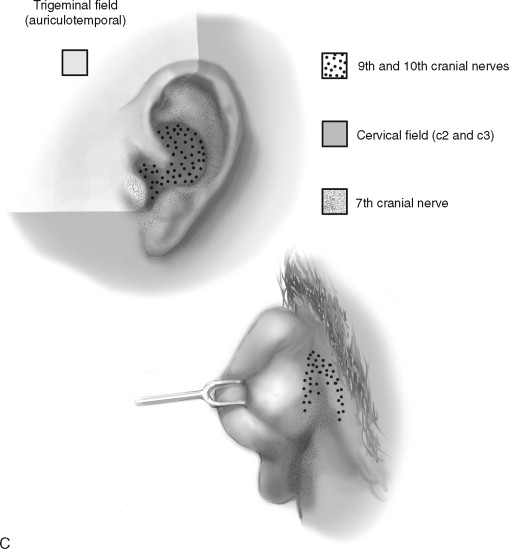
The sensory nerve supply is primarily from the anterior and posterior branches of the great auricular nerve. The nerve is an important surgical landmark, traveling 8 mm posterior to the postauricular crease. When dissecting in this area, care must be taken to avoid damage to the nerve, which can result in near complete anesthesia to the ear. Less-important contributions to sensation are made by the auriculotemporal and lesser occipital nerves to the conchal cavity and external auditory meatus ( Figure 32-5, B ). Regional anesthesia of the auricle is readily accomplished by instilling anesthetic solution along its base anteriorly and posteriorly ( Figure 32-6 ). Supplemental anesthesia may be needed at the posterior wall of the external auditory meatus supplied by the auricular branches of the vagus nerve (nerve of Arnold).
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


