This case report describes the treatment of a 37-year-old woman with multiple restored and missing teeth, a Class III subdivision malocclusion, and complete dental crossbite. Treatment options included orthognathic surgery and an orthodontic-prosthetic approach. The patient opted for nonsurgical treatment with space opening for prosthetic replacement of the first maxillary molars.
The treatment of adults with Class III malocclusion is a clinical challenge in orthodontics. With no maxillomandibular growth potential, adults have no treatment options except either orthognathic surgery or a nonsurgical compensatory approach. Surgical correction consists of mandibular setback, maxillary advancement, or a combination of mandibular and maxillary procedures. Nonsurgical treatment of a Class III malocclusion involves orthodontic treatment with compensation mechanics.
Patients with multiple restorations can have restorative treatment goals that complicate the orthodontic treatment. In adolescents with complete dentitions, orthodontic treatment objectives tend to be idealistic. In orthodontic-restorative patients, however, it is important to establish realistic, not idealistic, treatment objectives. As Kokich and Spear stated, treatment objectives should be economically realistic, occlusally realistic, and restoratively realistic.
This case report describes the treatment of an adult with many restored and missing teeth, a Class III subdivision malocclusion, and complete dental crossbite.
Diagnosis and etiology
A 37-year-old woman came for an orthodontic consultation with chief complaints of temporomandibular joint pain and an unesthetic smile. Her medical history showed no contraindication to orthodontic therapy. Her dental history included many restored teeth with previous endodontic therapy.
The extraoral examination ( Fig 1 ) indicated a straight to concave profile and marked nasolabial lines (suggesting maxillary retrusion) and a well-balanced face. Her forced smile had acceptable gingival display but suggested retroinclined maxillary incisors.
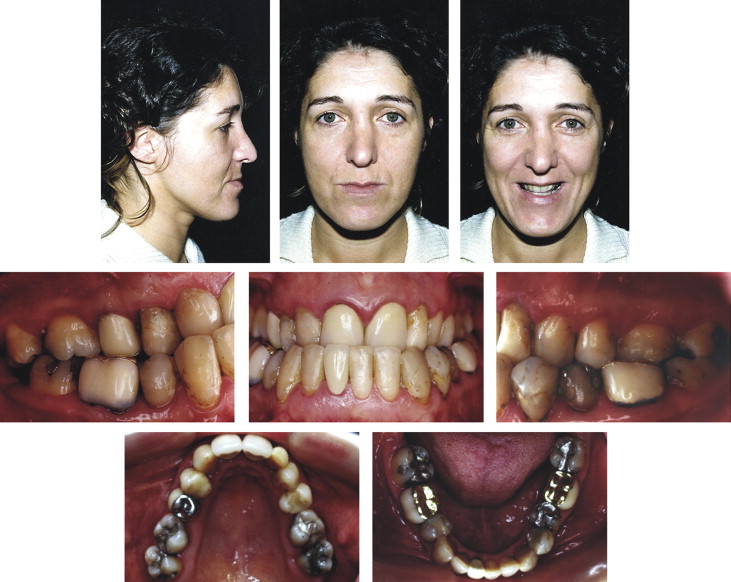
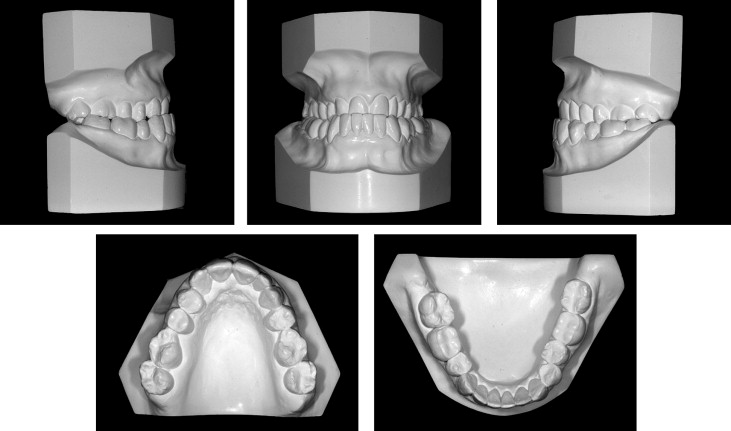
Intraoral ( Fig 1 ) and dental cast ( Fig 2 ) examinations showed several missing teeth in the maxilla (first molars, right lateral incisor, and left first premolar) and the mandible (third molars and right first premolar). All spaces between the teeth had closed. She had a Class III dental relationship on the right side and a Class I relationship on the left, as well as anterior and posterior crossbites. The maxillary midline was coincident with the facial midline, and the mandibular midline was shifted 4 mm to the right. There was no discrepancy between maximum intercuspation and centric relation.
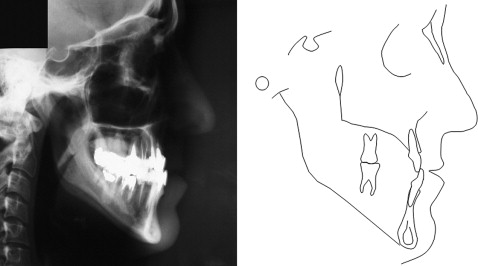
The lateral cephalogram and tracing ( Fig 3 ) showed a thin mandibular symphysis and mandibular incisors almost out of the bony crest. The cephalometric analysis ( Table ) indicated a vertical skeletal pattern (GoGn-SN, 45.0°; FMA, 37.0°; PFH, 51.0 mm; AFH, 79.0 mm; and FHI, 0.65) and a skeletal Class III relationship with maxillary retrusion (SNA, 70.0°, SNB, 73.0°; ANB, –3.0°; and AO-BO, –4.0 mm). The mandibular and maxillary incisors were retroinclined (FMIA, 66.0°; IMPA, 77.0°; 1.NB, 17.0°; 1-NB, 5.0 mm; 1.NA, 19.0°; 1-NA, 6.0 mm; and interincisal angle, 147.0°). She had a concave profile due to a more retruded maxilla (Z-angle, 78.0°; Pog-NB, 4.0 mm; S line-lower lip, 0.0 mm; S line-upper lip,–5.0 mm; and nasolabial angle, 94.0°). The panoramic radiograph ( Fig 4 ) showed many restored teeth. There were no evidence of bone or dental pathology and no defective restorations.
| Measurements | Average | Initial | Final | Prosthodontics |
|---|---|---|---|---|
| Skeletal | ||||
| SNA (°) | 82.0 | 70.0 | 71.0 | 71.0 |
| SNB (°) | 80.0 | 73.0 | 73.0 | 73.0 |
| ANB (°) | 2.0 | −3.0 | −2.0 | −2.0 |
| AO-BO (mm) | 2.0 | −4.0 | −5.0 | −5.0 |
| GoGn-SN (°) | 32.0 | 45.0 | 44.0 | 43.0 |
| Occ Pl-FH (°) | 10.0 | 7.0 | 7.0 | 7.0 |
| PFH (mm) | 45.0 | 51.0 | 53.0 | 53.0 |
| AFH (mm) | 65.0 | 79.0 | 78.0 | 77.0 |
| FHI (PFH/AFH) | 0.70 | 0.65 | 0.68 | 0.69 |
| FMA (°) | 25.0 | 37.0 | 36.0 | 35.0 |
| Dental | ||||
| FMIA (°) | 68.0 | 66.0 | 66.0 | 68.0 |
| IMPA (°) | 87.0 | 77.0 | 78.0 | 77.0 |
| 1.NB (°) | 25.0 | 17.0 | 17.0 | 17.0 |
| 1-NB (mm) | 4.0 | 5.0 | 5.0 | 5.0 |
| 1.NA (°) | 22.0 | 19.0 | 28.5 | 27.0 |
| 1-NA (mm) | 4.0 | 6.0 | 10.0 | 9.0 |
| Interincisal angle (°) | 131.0 | 147.0 | 136.0 | 138.0 |
| Soft tissues | ||||
| Z-angle (°) | 75.0 | 78.0 | 76.0 | 77.0 |
| Pog-NB (mm) | – | 4.0 | 4.0 | 4.0 |
| S line-lower lip (mm) | 0.0 | 0.0 | 0.0 | 0.0 |
| S line-upper lip (mm) | 0.0 | −5.0 | −1.0 | −2.0 |
| Nasolabial angle (°) | 100.0 | 94.0 | 92.0 | 94.0 |

Treatment objectives
The ideal treatment objectives were to correct the skeletal discrepancies between the maxilla and the mandible, resolve the anterior and posterior crossbites, establish satisfactory overbite and overjet, correct the mandibular midline, align and correct the rotations, obtain a stable occlusal relationship, and improve the patient’s facial and dental esthetics.
Because this adult patient had multiple restorations with a vertical and Class III skeletal pattern as well as a thin mandibular symphysis, the realistic treatment objectives were to (1) establish a functional occlusion and mitigate the temporomandibular disorder symptoms, (2) establish satisfactory overbite and overjet, (3) correct the anterior and posterior crossbites, (4) improve facial esthetics, and (5) provide an esthetic smile.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


