Fig. 8.1
Clinical aspect of chronic hyperplastic candidosis at the commissures and oral mucosa

Fig. 8.2
Clinical appearance of plaque-like lesion of right commissural and retrocommissural area

Fig. 8.3
Chronic hyperplastic candidosis at the commissural and retrocommissural area

Fig. 8.4
Plaque-like lesion at the commissural and retrocommissural region in oral mucosa
Diagnosis
In general, the diagnosis of oral candidosis is based on clinical signs and symptoms in conjunction with a complete medical history. Clinical diagnosis is usually confirmed by laboratory tests from clinical samples (Farah et al., 2010). Oropharyngeal swab cultures may demonstrate Candida spp., but, because colonization of the oral mucosa by Candida is common, this is not necessarily diagnostic. Confirmation of a diagnosis of oral candidosis can be accomplished via a 10 % potassium hydroxide slide preparation of a mucosal scraping from a suggestive oral lesion (Thompson et al., 2010). Often, a biopsy is required to establish the diagnosis of oral hyperplastic chronic candidosis and to rule out other white lesions.
Histopathological Characteristics
The histopathological characteristics of CHC may vary according to their clinical presentation. The candida infection not only causes epithelial hyperplasia, but can also induce epithelial atypias (Shibata et al., 2011).
The following histopathologic features can be found in cases of oral hyperplastic chronic candidosis:
-
Hyperplasia of the rete ridges (Fig. 8.5)
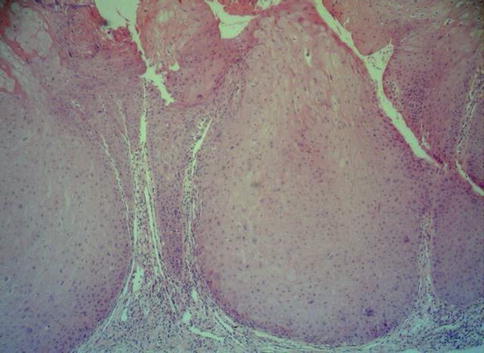 Fig. 8.5Histopathological aspect of chronic hyperplastic candidosis – epithelial hyperplasia (HE ×10)
Fig. 8.5Histopathological aspect of chronic hyperplastic candidosis – epithelial hyperplasia (HE ×10) -
Hyperorthokeratinized or hyperparakeratinized mucosa (Fig. 8.6)
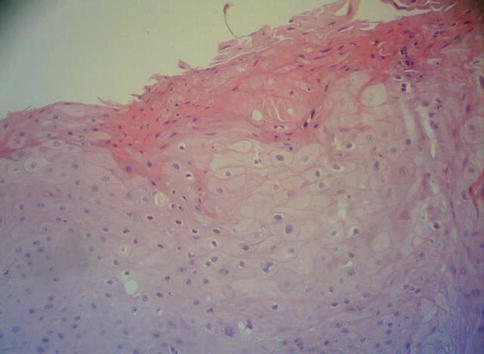 Fig. 8.6Histopathological aspect of chronic hyperplastic candidosis – hyperparakeratosis (HE ×100)
Fig. 8.6Histopathological aspect of chronic hyperplastic candidosis – hyperparakeratosis (HE ×100) -
Chronic inflammatory cells infiltrate (Fig. 8.7)
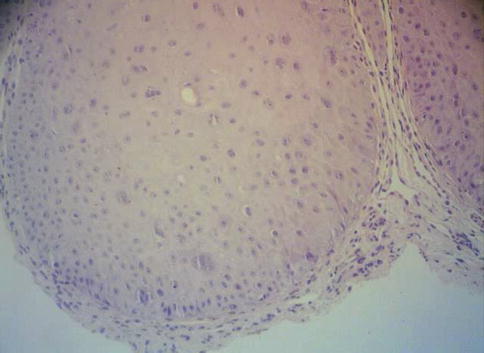 Fig. 8.7Homogenous chronic hyperplastic candidosis – epithelial dysplasia, acanthosis, hyperchromatism, and chronic inflammatory cell infiltrate in the lamina propria (HE ×100)
Fig. 8.7Homogenous chronic hyperplastic candidosis – epithelial dysplasia, acanthosis, hyperchromatism, and chronic inflammatory cell infiltrate in the lamina propria (HE ×100) -
Acanthosis (Fig. 8.7)
-
Epithelial dysplasia (Fig. 8.7)
-
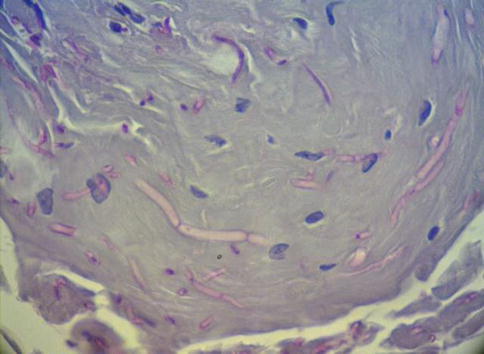
Dyskeratoses (Fig. 8.8)
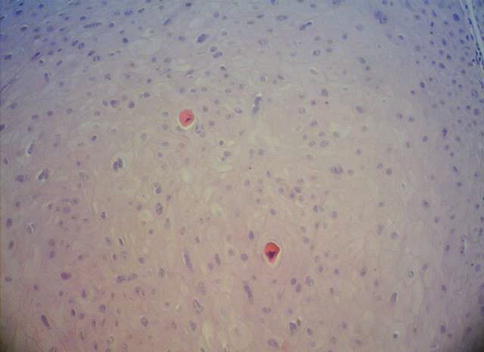 Fig. 8.8Homogenous chronic hyperplastic candidosis – dyskeratoses (HE ×100)
Fig. 8.8Homogenous chronic hyperplastic candidosis – dyskeratoses (HE ×100)
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


