Chapter 11 Oral appliance and craniofacial problems of obstructive sleep apnea syndrome
1 INTRODUCTION
Pierre Robin (1934) used the monoblock mandible advancement appliance for the purpose of treating patients with obstructive sleep apnea for the first time.1 Following this, Boraz treated pediatric OSA patients.2 Cartwright and Samelson (1982)3 reported the effectiveness of the tongue retaining device (TRD) which retains the tongue in the bulb of the device. Meier-Ewert (1984)4 used Esmarch–Heiberg manipulation, which opens the airway of a general anesthetized patient, and developed the Esmarch appliance. The tongue retaining appliance represented by the TRD, and the mandible advancing type represented by the Esmarch, are the two main types of oral appliance. Thereafter, other oral appliances were developed such as the adjustable type, which can adjust the amount of mandible advancement. Currently, more than 55 oral appliances (OAs) are on the market.5
2 PATIENT SELECTION
In 2006, the Standards of Practice Committee of the American Academy of Sleep Medicine published the reports Oral Appliance for Snoring and Obstructive Sleep Apnea: A Review6 and Practice Parameters for the Treatment of Snoring and Obstructive Sleep Apnea with Oral Appliances: An Update for 2005.7 Oral appliances are indicated for use with patients with primary snoring and with mild to moderate OSA, who prefer them to continuous positive airway pressure (CPAP) therapy, or who do not respond to CPAP, are not appropriate candidates for CPAP, or who have failed treatment attempts with CPAP.
3 PROCEDURES FOR ORAL APPLIANCE THERAPY
The procedures for oral appliance therapy are as follows.
4 ORAL APPLIANCE VARIATIONS


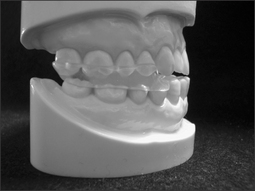
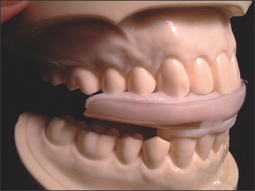
4.2 MANDIBULAR ADVANCING TYPE
4.2.1 NON-TITRATABLE TYPE

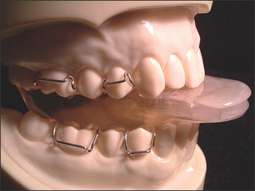

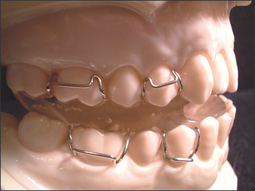


4.2.2 TITRATABLE TYPE
The mandibular advancing and titratable type of oral appliance is a custom-made two-piece appliance composed of two separate arches (maxillary and mandibular) containing an advancing mechanism. Examples are listed below.
< div class='tao-gold-member'>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


