Chapter 64 Obstructive sleep apnea in children with adenotonsillar hypertrophy
Obstructive sleep apnea (OSA) is a common and serious cause of morbidity during childhood. It affects 1−3% of children of 2−8 years old. However, habitual snoring during sleep is a much more frequent occurrence and affects up to 27% of children, with a decrease in frequency in 9 to 14 year olds. OSA in children presents some characteristics which differ from those in adults. Adenotonsillar hypertrophy (Fig. 64.1) is the most frequent causative disease according to our recent experience (Table 64.1). In addition, OSA results in some specific features (Table 64.2), which may only be observed in children. Furthermore, the correlation between OSA and sudden infant death syndrome (SIDS), and ALTE (apparent life-threatening event) in infants should be addressed further.
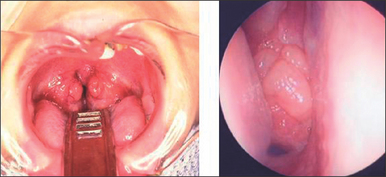
Table 64.1 The causative diseases of obstructive sleep dyspnea in children
| Hypertrophy of tonsil and adenoid | 88.9% |
| Habitual angina | 3.7% |
| Nasal allergy | 2.5% |
| Sudden infant death syndrome | 1.2% |
| Hunter–Hurler syndrome | 1.2% |
| Niemann–Pick’s disease | 1.2% |
| Prader–Willi syndrome | 1.2% |
Table 64.2 Typical features of OSA in children
| Adenoid face |
| Mouth-breathing |
| Chest deformity (Fig. 64.2) |
| Snoring and apnea |
| Supraclavicular and intercostals retractions |
| Sweating |
| Late awaking, or forced awaking |
| Longer daytime sleep, sleepiness |
| Late asleep |
| Sudden awakening |
| Bed wetting or its recurrence |
| Abnormal behavior |
| Poor academic achievement |
1 DIAGNOSIS OF DYSPNEA IN CHILDREN
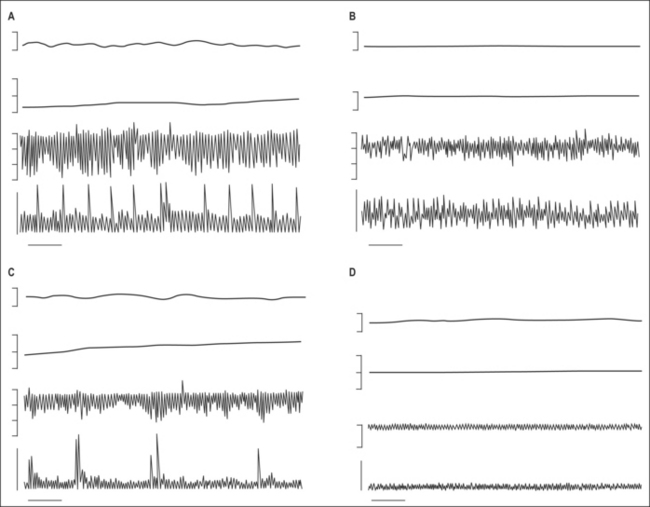
Polysomnographic diagnosis is usually necessary for adults, in whom clinical symptoms will be presented when there are more than five apneas per hour, or over 30 times in 7 hours of sleep. In the case of children, apnea-like symptoms may be observed even when there is continuous hypoventilation, but not a typical apnea. We measured the esophageal pressure (Peso) to evaluate the respiratory efforts in children with adenotonsillar hypertrophy and OSA, and discovered that the degree of Peso increased even without apnea when in deep sleep (Fig. 64.3). Therefore, because the measurement of polysomnography (PSG) in a child is difficult, and also because of the specific characteristic of children’s OSA, the diagnostic criterion of PSG is still unclear in children, especially in infants.
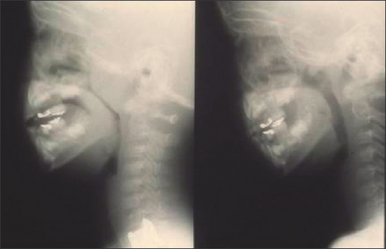
Monitoring oxygen saturation during sleep seems to be valid. The degree of stenosis in airways can be detected by profile roentgen film (Fig. 64.4), or by direct observation under a thin flexible fiberscope. A video camera is nowadays available in many families. A video record is also useful in observing respiratory situations, and even in cases without obvious desaturation, apnea could be found.
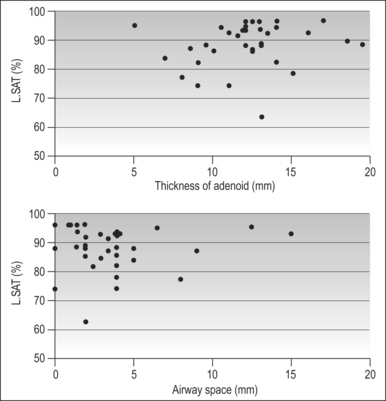
In 37 children with adenotonsillar hypertrophy, we inv estigated the thickness of adenoid, size of the airway space, and the lowest saturation during sleep. The lowest saturation was correlated to neither adenoid thickness nor airway space (Fig. 64.5). The grade of upper airway stenosis by adenoid or tonsillar hypertrophy on profile roentgen films could not predict the severity of apnea during sleep. For precise diagnosis of respiratory severity caused by adenoid–tonsillar hypertrophy, video observation with simultaneous SpaO2 monitoring is necessary. However, this result did not suggest that roentgenic measurement of stenosis is meaningless. When severe hypertrophy of the tonsil and adenoid is recognized, the possible existence of respiratory impairment should be investigated out of caution. Even in cases with moderate hypertrophy, severe apnea could be a possible accompaniment.
On the other hand, the adenoid and tonsil keep growing after birth until around 8 years old. Although the airway space in the pharynx also becomes larger, the ratio of adenotonsillar thickness to airway space reaches its peak at 4–6 years old. A previous study pointed out that children with OSA showed severe hypertrophy at younger ages (less than 3 years), which differed significantly compared to physiological hypertrophy of normal children (Fig. 64.6). Earlier surgical treatments are necessary for these cases.
< div class='tao-gold-member'>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


