A woman was referred to the orthodontic clinic for treatment. She was diagnosed with a skeletal Class II malocclusion, a steep mandibular plane, and an anterior open bite. Conventional orthodontic treatment was considered to correct the maxillary protrusion and anterior open bite, but the patient also requested improvement of her facial esthetics. We therefore decided that nonsurgical treatment consisting of 4 premolar extractions combined with temporary anchorage devices was indicated. Satisfactory improvement of the overjet and overbite, and proper functional occlusion were obtained, resulting in a Class I molar relationship. Active treatment was completed in 2 years 10 months, and the result remained stable at 2 years 6 months after debonding.
Highlights
- •
Treatment of Class II malocclusion with steep mandible and anterior open bite is reported.
- •
The treatment was nonsurgical with 4 premolar extractions combined with temporary anchorage devices.
- •
Proper functional occlusion was obtained.
- •
The profile was changed from convex to almost straight.
- •
The results remained stable at 2 years 6 months after retention.
Orthodontists often encounter various types of open-bite malocclusions in adult patients. Open-bite malocclusion can be corrected by conventional orthodontic methods, orthodontic treatment combined with temporary anchorage devices (TADs), or orthognathic surgery. Recently, TADs have been developed and are indicated for various orthodontic conditions. The major applications of TADs in orthodontic treatment are intrusion or distal movement of the molars. The morphologic characteristics of open bite are a steep mandibular plane, thin and long morphology of the mandibular symphysis, and increased anterior facial height. Orthodontic treatment combined with TADs, as well as surgical orthodontic treatment, might improve facial esthetics without increasing the anterior facial height.
In this case report, we demonstrate a nonsurgical orthodontic treatment of an adult with a skeletal Class II anterior open bite and a large Frankfort-mandibular plane angle (FMA). Since the patient desired improvement of her facial esthetics along with a suitable occlusion by undergoing orthodontic treatment alone, nonsurgical treatment combined with TADs was applied.
Diagnosis and etiology
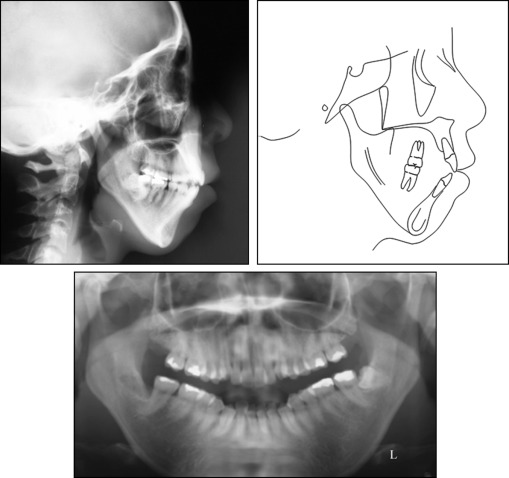
The patient was a 28-year-old Japanese woman with an anterior open bite and crowding. She was in good health and had no contraindications for dental treatment. No facial asymmetry was evident in the frontal view of the face. She had a convex facial profile with increased anterior lower facial height and upper lip protrusion with incompetent lips ( Fig 1 ). She had an anterior open bite and anterior crowding in both arches. The molar relationship was Angle Class II subdivision on the right. Overjet and overbite were +2.5 and −0.5 mm, respectively. Both arches were narrow in the molar regions ( Fig 2 ). The cephalometric analysis showed a skeletal Class II malocclusion (ANB, 7.0°) with a long face, and the morphology of the mandibular symphysis was thin and long. The maxillary and mandibular incisors had a lingual inclination (maxillary central incisor to SN, 92.5°) and an incisor-mandibular plane angle (IMPA) of 82.0° ( Table ). The patient was diagnosed with a skeletal Class II malocclusion with a steep mandibular plane, anterior open bite, and crowding. She had a history of treatment for temporomandibular joint disorder, but the pretreatment panoramic radiograph showed no bony change of the condylar heads bilaterally ( Fig 3 ).


| Measurement | Pretreatment | Posttreatment | Postretention |
|---|---|---|---|
| Angular (°) | |||
| SNA | 76.0 | 76.0 | 76.0 |
| SNB | 69.0 | 70.0 | 70.0 |
| ANB | 7.0 | 6.0 | 6.0 |
| Facial angle | 74.0 | 76.0 | 76.0 |
| Convexity | 18.5 | 17.0 | 17.5 |
| FMA | 54.0 | 53.0 | 53.5 |
| Y-axis | 76.0 | 75.5 | 76.0 |
| Gonial angle | 148.0 | 148.0 | 148.5 |
| Occlusal plane to Frankfort horizontal | 19.5 | 20.0 | 20.0 |
| U1-SN | 92.5 | 93.0 | 92.0 |
| IMPA | 82.0 | 74.0 | 73.5 |
| FMIA | 44.0 | 53.0 | 53.0 |
| Interincisal angle | 122.5 | 129.0 | 131.0 |
| Linear (mm) | |||
| Overjet | 3.0 | 2.0 | 2.0 |
| Overbite | −0.5 | 2.0 | 2.0 |
| U-1 to A-P pog | 11.0 | 9.0 | 9.0 |
| L-1 to A-P pog | 9.0 | 6.0 | 6.0 |
| N-ANS | 56.0 | 56.0 | 56.0 |
| ANS-Ne | 79.0 | 78.0 | 78.0 |
Treatment alternatives
Two treatment options were considered for this patient: (1) surgical orthodontic treatment, which could improve both occlusion and facial appearance, was the primary treatment plan of choice; or (2) nonsurgical orthodontic treatment with extraction of the maxillary first premolars and mandibular second premolars combined with TADs for the maxilla and mandible was considered as an alternative to orthognathic surgery.
These alternatives were discussed with the patient. TADs would be used to intrude the maxillary and mandibular molars, resulting in a change in facial appearance. Since the patient refused surgical orthodontic treatment, conventional orthodontic treatment with TADs was adopted.
The predicted treatment outcome was explained to the patient, and informed consent was obtained.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


