Armamentarium
|
History of the Procedure
Originally based on the halstedian principles of en bloc removal of lymph nodes in the neck, neck dissection is a standard procedure for the management of patients with head and neck tumors. The term neck dissection has evolved to encompass several different forms of the procedure, which may be selected based on the nature of the patient’s disease. Neck dissection was first described in the late nineteenth century by von Langenbeck, Billroth, von Volkmann, and Kocher, who developed and reported the early cases of different types of neck dissection. Butlin, in England, developed the concept of elective neck dissection. However, it was George Crile, in 1906, who reported the first significant series of cases on radical neck dissection, bringing this procedure to the attention of the medical world as an effective operation with reproducible techniques and results.
The greatest impetus to the status of this surgical procedure came from Martin et al. In 1951, these researchers published a monumental report of 1,450 cases that established the place and technique of radical neck dissection in the modern treatment of head and neck cancer. The traditional radical neck dissection now is reserved for patients with bulky metastatic neck disease and those with a regional failure after a more limited neck dissection. In 1967, Bocca described the concept of a functional neck dissection with limited surgical morbidity, for which the oncologic safety was equivalent to that of a radical neck dissection.
History of the Procedure
Originally based on the halstedian principles of en bloc removal of lymph nodes in the neck, neck dissection is a standard procedure for the management of patients with head and neck tumors. The term neck dissection has evolved to encompass several different forms of the procedure, which may be selected based on the nature of the patient’s disease. Neck dissection was first described in the late nineteenth century by von Langenbeck, Billroth, von Volkmann, and Kocher, who developed and reported the early cases of different types of neck dissection. Butlin, in England, developed the concept of elective neck dissection. However, it was George Crile, in 1906, who reported the first significant series of cases on radical neck dissection, bringing this procedure to the attention of the medical world as an effective operation with reproducible techniques and results.
The greatest impetus to the status of this surgical procedure came from Martin et al. In 1951, these researchers published a monumental report of 1,450 cases that established the place and technique of radical neck dissection in the modern treatment of head and neck cancer. The traditional radical neck dissection now is reserved for patients with bulky metastatic neck disease and those with a regional failure after a more limited neck dissection. In 1967, Bocca described the concept of a functional neck dissection with limited surgical morbidity, for which the oncologic safety was equivalent to that of a radical neck dissection.
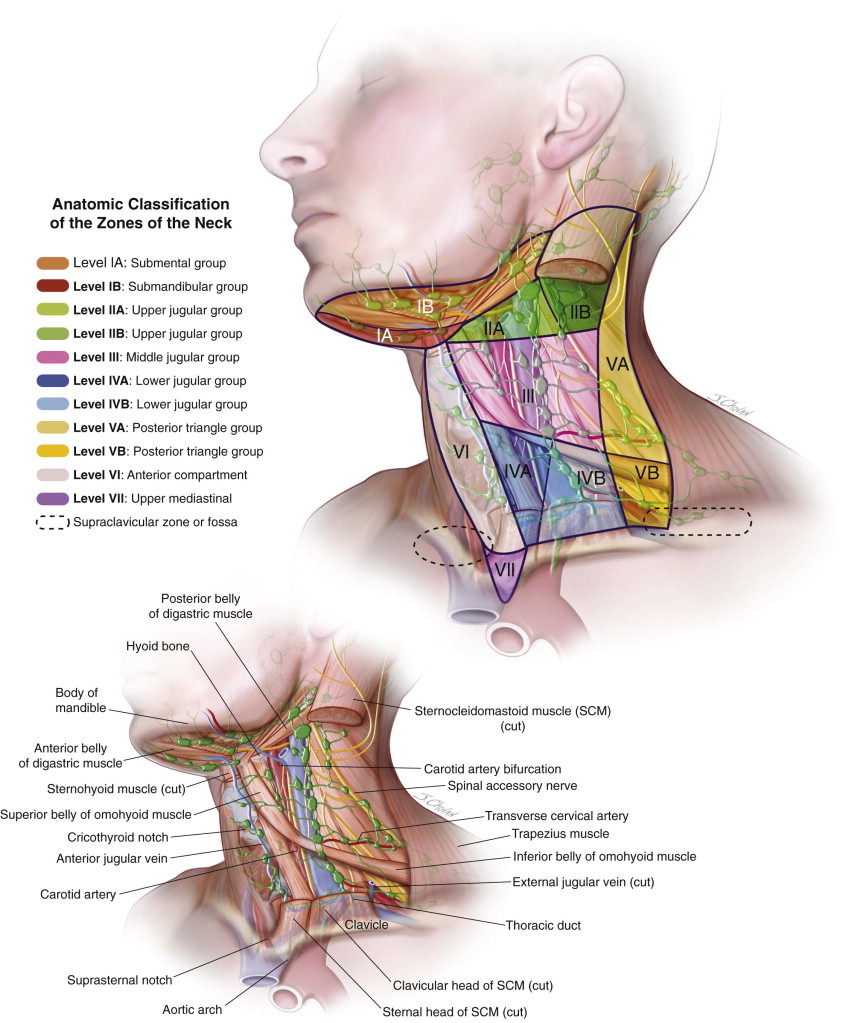
Anatomic Classification of the Zones of the Neck
The lymph node basins in the neck have been described in various levels, first by Memorial Sloan Kettering; they were then further subdivided by Suen and Goepfert at MD Anderson. The anatomic basis of neck node level classifications provides the basis for surgical extirpation of lymph node areas of the neck based on the origin and first echelon lymphatic drainage system, according to the site of the primary tumor. Figure 103-1 shows the different zones and levels of the neck.
Boundaries:
- •
Anterior—Lateral border of the sternohyoid muscle
- •
Posterior—Posterior border of the sternocleidomastoid muscle
- •
Superior—Skull base
- •
Inferior—Level of the hyoid bone (clinical landmark) or carotid bifurcation (surgical landmark)
Levels IIa and IIb are arbitrarily designated anatomically by splitting level II with the spinal accessory nerve.
Boundaries:
- •
Anterior—Lateral border of the sternohyoid muscle
- •
Posterior—Posterior border of the sternocleidomastoid muscle
- •
Superior—Hyoid bone (clinical landmark) or carotid bifurcation (surgical landmark)
- •
Inferior—Cricothyroid notch (clinical landmark) or omohyoid muscle (surgical landmark)
Boundaries:
- •
Anterior—Lateral border of the sternohyoid muscle
- •
Posterior—Posterior border of the sternocleidomastoid muscle (SCM)
- •
Superior—Cricothyroid notch (clinical landmark) or omohyoid muscle (surgical landmark)
- •
Inferior—Clavicle
Level IVa denotes the lymph nodes that lie along the internal jugular vein but immediately deep to the sternal head of the SCM. Level IVb denotes the lymph nodes that lie deep to the clavicular head of the SCM.
Boundaries:
- •
Anterior—Posterior border of the sternocleidomastoid muscle
- •
Posterior—Anterior border of the trapezius muscle
- •
Inferior—Clavicle
Level Va denotes lymphatic structures in the upper part of level V that follow the spinal accessory nerve. Level Vb refers to nodes that lie along the transverse cervical artery. Anatomically, the division between these two subzones is the inferior belly of the omohyoid muscle.
Boundaries:
- •
Lateral—Carotid sheath
- •
Superior—Hyoid bone
- •
Inferior—Suprasternal notch
Boundaries:
- •
Lateral—Carotid arteries
- •
Superior—Suprasternal notch
- •
Inferior—Aortic arch
Supraclavicular zone or fossa (relevant to nasopharyngeal carcinoma)
Boundaries:
- •
Superior margin of the sternal end of the clavicle
- •
Superior margin of the lateral end of the clavicle
- •
The point where the neck meets the shoulder
Classification of Neck Dissection
In 1991, the Committee for Head and Neck Surgery and Oncology of the American Academy of Otolaryngology/Head and Neck Surgery developed a classification system for neck dissections. Before then and since, other authors have proposed other classification systems; however, the academy’s system remains the most widely accepted and has been endorsed by the American Society for Head and Neck Surgery. It is based on the following concepts.
- 1.
Radical neck dissection (RND) is the standard basic procedure for cervical lymphadenectomy. It involves removal of the lymph nodes in levels I through V with sacrifice of the sternocleidomastoid muscle (SCM), internal jugular vein (IJV), and spinal accessory nerve (cranial nerve [CN] XI).
- 2.
Modified radical neck dissection (MRND) involves the preservation of any nonlymphatic structures while maintaining nodal sampling in levels I through V.
- 3.
Selective neck dissection (SND) is any procedure that preserves one or more groups or levels of lymph nodes:
- •
Supraomohyoid type (levels I through III)
- •
Lateral type (levels II through IV)
- •
Posterolateral type (levels II through V)
- •
Anterior compartment type (level VI)
- •
- 4.
An extended neck dissection (END) refers to the removal of additional lymph node groups or nonlymphatic structures relative to the radical neck dissection.
In 1989, Medina suggested that the term “comprehensive neck dissection” be used whenever all the lymph nodes in levels I through V are removed. He recommended three subtypes of modified radical neck dissection:
- •
Type I (CN XI preserved)
- •
Type II (CN XI, IJV preserved)
- •
Type III (CN XI, IJV, and SCM preserved)
Indications for the Use of the Procedure
Neck dissection is indicated in most patients with head and neck cancer. The primary goal of neck dissection can be pathologic staging of the neck, to determine whether further therapy is warranted with a clinically staged N0 neck. Alternatively, neck dissection can be performed as a therapeutic procedure for patients with evidence of metastatic disease either clinically or pathologically.
Radical neck dissections typically are reserved for patients with bulky N3 neck disease, in which oncologic safety cannot be obtained with preservation of the nonlymphatic structures of the SCM, IJV, or spinal accessory nerve. MRND is indicated in patients with clinical or radiographic evidence of nodal metastasis to the neck that does not directly infiltrate or adhere to the nonlymphatic structures, which can be preserved.
The basis on which supraomohyoid neck dissection (SOHND) was developed for treatment of the N0 neck in patients with oral cavity carcinomas was established in 1972 by Lindberg in a study that examined the distribution of lymph node metastasis in head and neck squamous cell carcinomas. He showed that the level II midjugular nodes were the most likely affected lymphatics.
SND is indicated for patients who have primary tumors arising from the oral cavity without clinical or radiologic evidence of cervical metastasis, but who have a high probability of occult lymphatic disease. Kligerman established the basis of SND with a risk of occult metastasis of greater than 20%. The therapeutic implications are that all patients with tumors graded T2 or higher and those who have an oral cavity tumor with a thickness greater than 3 to 4 mm exceed the relative risk of 20% of occult metastasis and should be considered for SND.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


