Chapter 50 Multilevel surgery (hyoid suspension, radiofrequent ablation of the tongue base, uvulopalatopharyngoplasty) with/without genioglossal advancement
1 INTRODUCTION
Severe obstructive sleep apnea syndrome (OSAS) is preferably treated by nasal continuous positive airway pressure (NCPAP). Unfortunately, 30–50% of patients refuse or cannot accept NCPAP for a variety of reasons. Approximately 25% of patients refuse upfront or cannot pass the test period, others cannot accept or refuse it in the long run, or use it for only a few hours per night and/or less than 5 nights per week. It is our experience that increasingly many – especially young – patients refuse NCPAP therapy upfront and ask how realistic surgical alternatives are. Whatever the reason for not using NCPAP, treatment remains indicated in patients with severe OSAS and NCPAP refusal/failure. Many invasive alternatives are being explored. Various surgical interventions are available, such as uvulopalatopharyngoplasty (UPPP), Z-PP, uvula flap and other variations, in case of palatal obstruction, and hyoid suspension (HS) and genioglossal advancement (GA), in retrolingual obstruction. Maxillomandibular advancement (MMA) and tracheostomy are usually very effective, but the morbidity of these two modalities limits their application in the first line of surgery. In addition to surgical modalities, minimally invasive interventions exist, such as radiofrequent thermotherapy of palate and/or tongue base (RFTB). Surgery can be divided into unilevel (at palatinal or tongue base level only) and multilevel (surgery at both these levels), and can be performed either staged, or in one surgical event. Nose and nasopharynx in this regard are less important, in that where no nasal blockage is present, it has been shown that there is little use in increasing nasal airflow.
3 PATIENTS AND METHODS
All patients who visited our department from July 2003 to June 2005 because of habitual snoring and/or suspicion of sleep apnea syndrome were evaluated by history, physical examination, full overnight polysomnography and either by midazolam or propofol-induced sedated endoscopy. Patients with moderate to severe OSAS, both retrolingual and retropalatinal narrowing or collapse at sedated endoscopy, and refusal or non-acceptance of NCPAP treatment were offered a multilevel surgical approach. Full night sleep registration was performed preoperatively and 3 months postoperatively (see Chapter 49: Hyoid suspension as only procedure).
3.1 TREATING OBSTRUCTION AT PALATINAL LEVEL
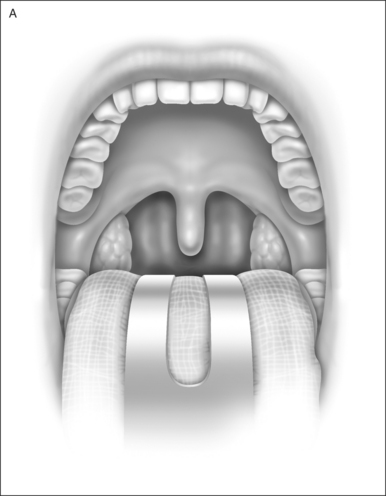
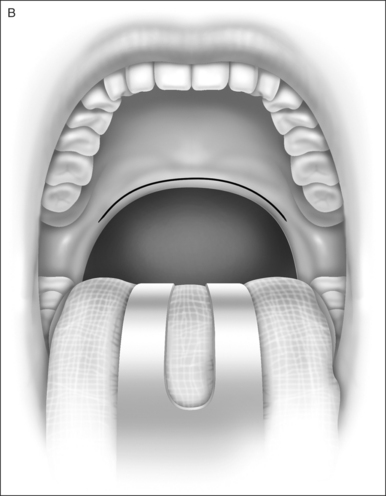
Uvulopalatopharyngoplasty was performed according to Fujita’s technique; the anterior and posterior tonsillar pillars were trimmed and reoriented, and the uvula was excised to create more retropalatinal space (Fig. 50.1). Tonsillectomy was performed if it had not been donepreviously (in 15 of 22 [68%] patients). In patients whohad had tonsillectomy previously, with a short anterior posterior diameter at retropalatinal level, Z-PP according to Friedman was performed (see Chapter 33).
3.2 TREATING OBSTRUCTION AT TONGUEBASE LEVEL
3.2.1 RADIOFREQUENT ABLATION OF THE TONGUE BASE (BIPOLAR, CELON®)
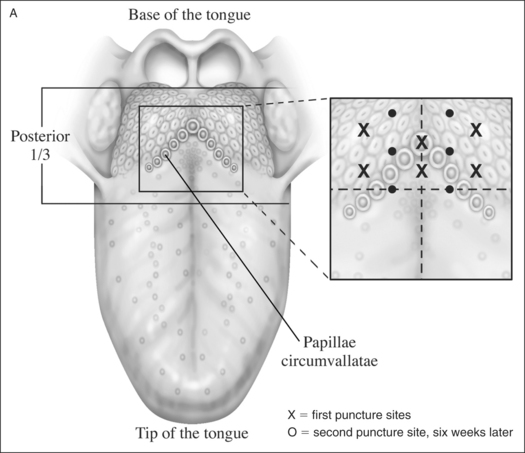
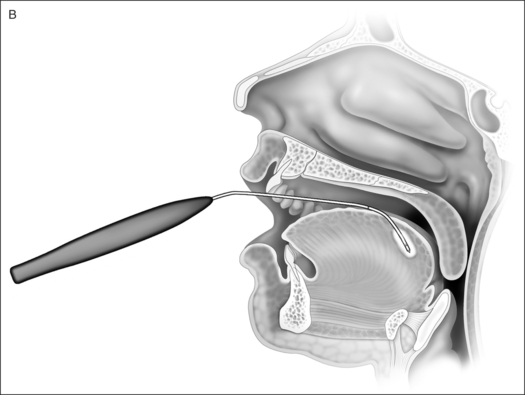
This was used for stiffening of the base of tongue. Energy was delivered with an exclusive needle device through the dorsal surface of the tongue. Evidence-based criteriafor technical adjustment and optimal energy dosageaccording to relevant increase in lesion size were used. After the initial surgical procedure, on indication a second and sometimes third additional RFTB was performed(Fig. 50.2).
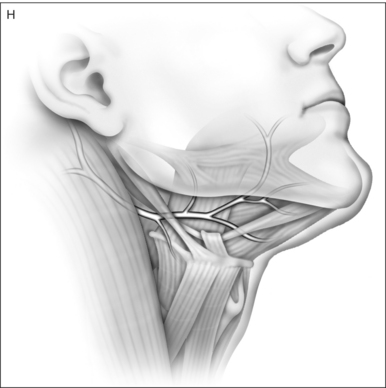
3.2.2 HYOID SUSPENSION
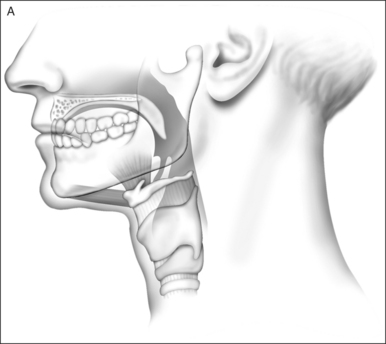
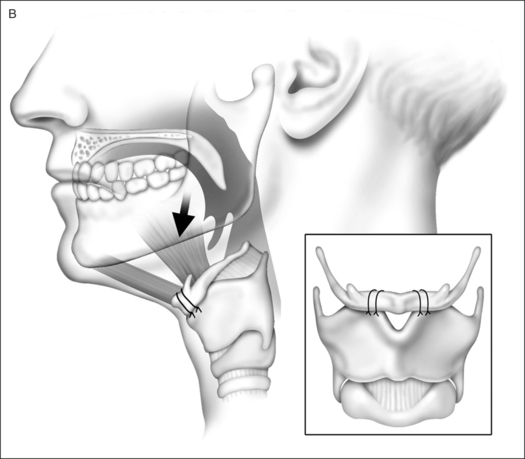
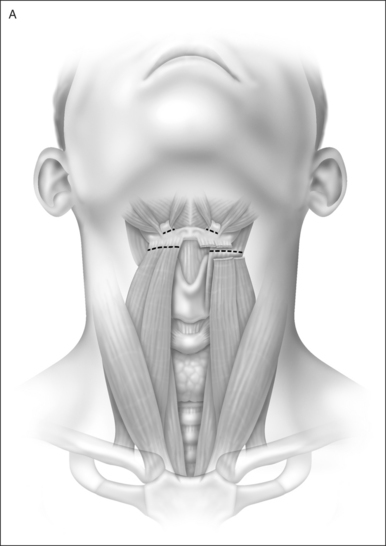
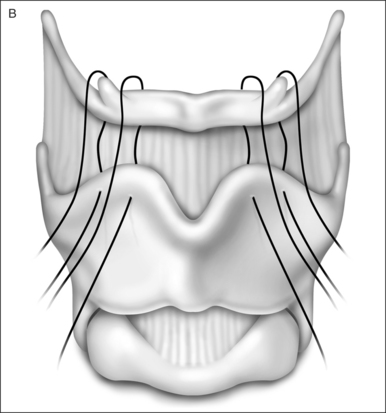
After exposure via an external horizontal incision at the level of the membrana thyrohyoidea, the strap muscles(M. sternohyoideus, M. omohyoideus and M. thyrohyoideus) were divided just below the hyoid and superior to the hyoid the tendon of the stylohyoideus was divided from the hyoid bone (Fig. 50.3) (for details see Chapter 49: Hyoid suspension as only procedure).
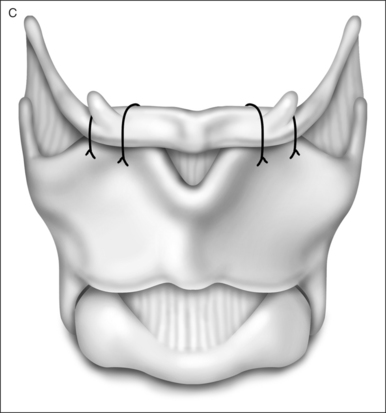
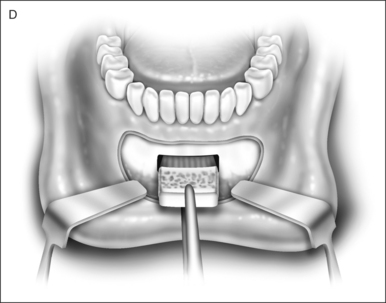
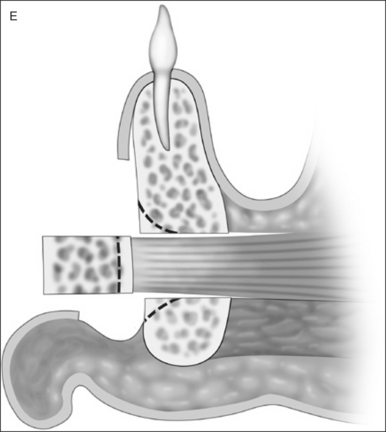
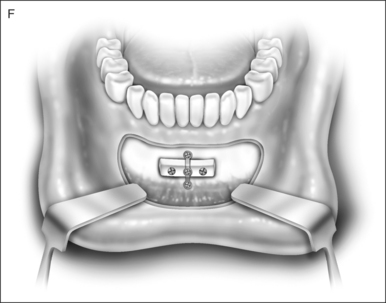
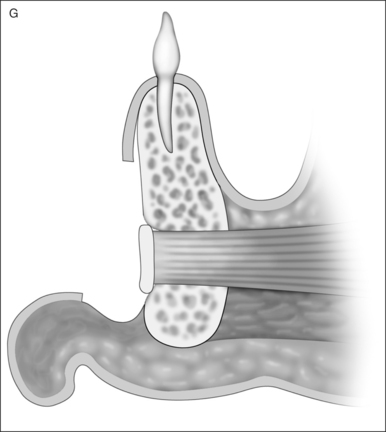
3.2.3 GENIOGLOSSUS ADVANCEMENT
A standard anterior mandibular osteotomy, limited to advancement of a rectangular window of the mandible including the genial tubercle and genioglossus musculature, but without rotation of the segment, was performed. The outer cortex and medulla were removed, the lingual cortical plate advanced and fixed with bone screws (Fig. 50.4).
< div class='tao-gold-member'>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


